If youve just heard the term mitral valve regurgitation for the first time, you might be feeling a mix of curiosity and worry. The good news is that you dont have to navigate this alone, and you certainly dont need to panic. In most cases, treatment is tailored to how big the leak is and how your heart is handling it. Below, Ill walk you through everything you need to knowfrom spotting the early signs to deciding whether medication, surgery, or a minimallyinvasive procedure is right for you.
Understanding the Diagnosis
What is mitral valve regurgitation?
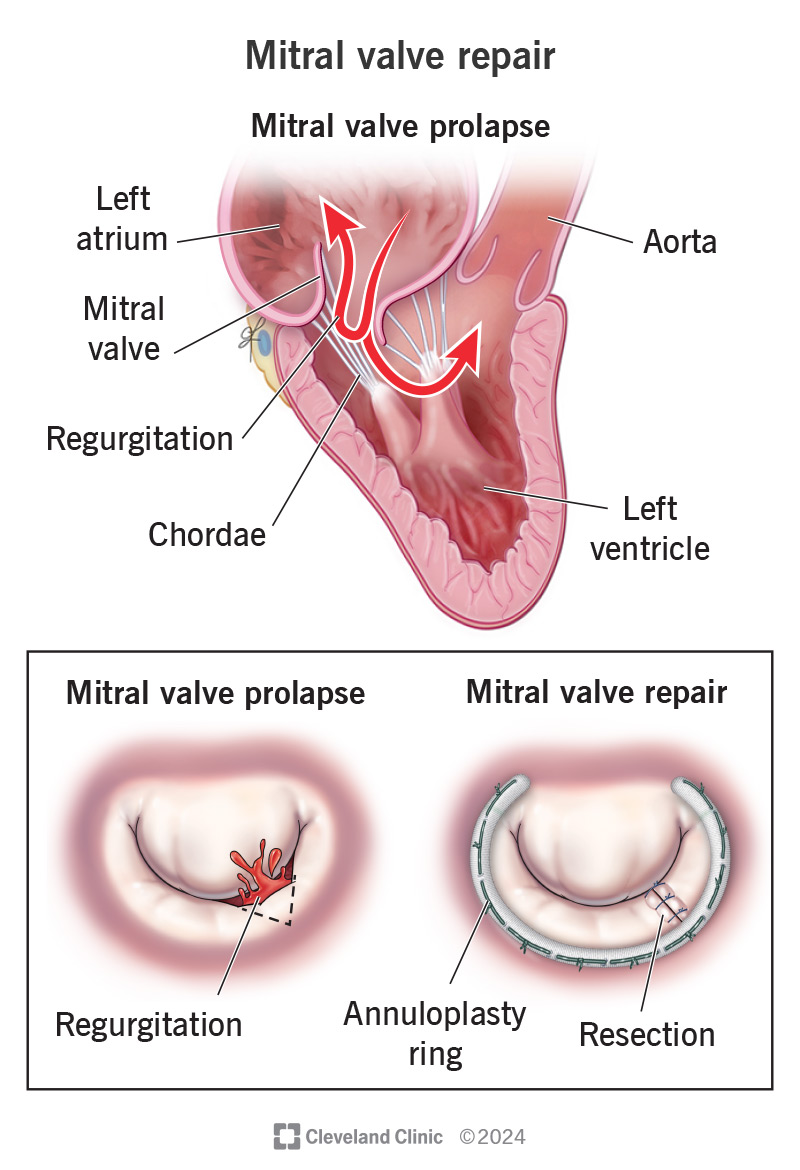
The mitral valve sits between the left atrium and left ventricle, acting like a oneway door that lets blood flow forward and prevents it from slipping back. When that door doesnt close tightly, blood leaks backwarda condition we call mitral valve regurgitation. Think of it as a leaky faucet; the more water that drips back, the harder the pump (your heart) has to work.
How is severity graded? (Grades12 vs34)
Doctors use echocardiograms to measure how much blood is flowing backward. The results fall into grades:
- Grade12 (mild): Small leak, often asymptomatic.
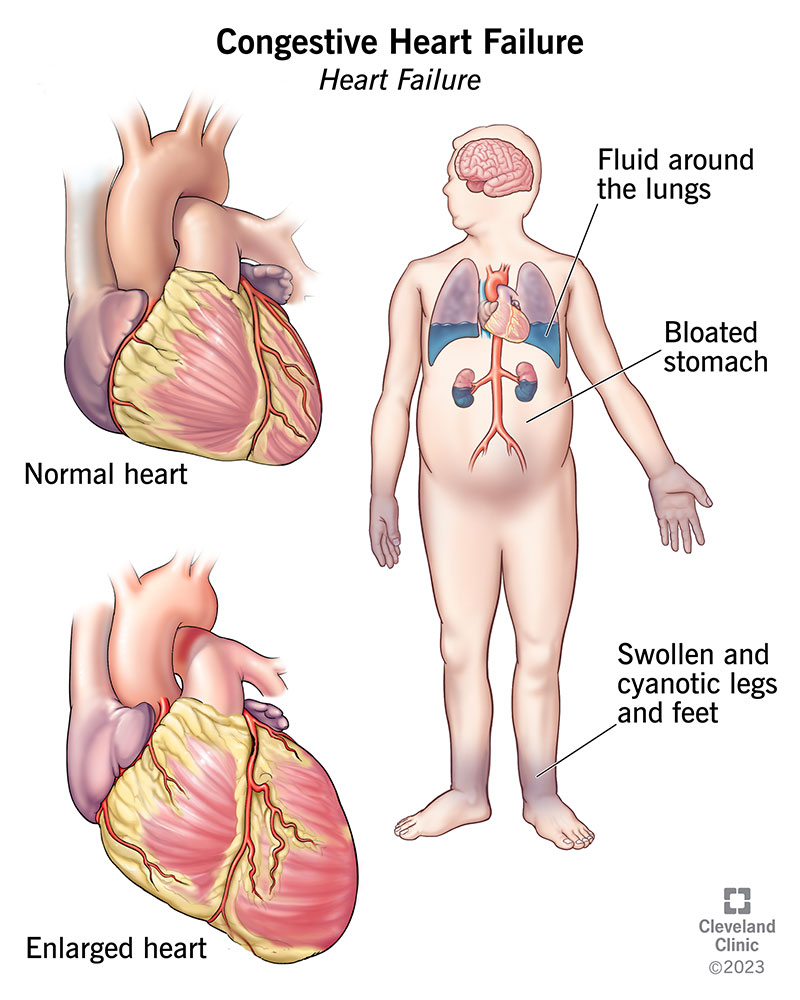
- Grade34 (moderate to severe): Larger leak, can cause fatigue, shortness of breath, or even heart failure.
Typical echo measurements
| Grade | Regurgitant Volume (ml/beat) | EROA (cm) |
|---|---|---|
| 12 (Mild) | <30 | <0.2 |
| 34 (ModerateSevere) | 30 | 0.2 |
How fast does mitral valve regurgitation progress?
Most people wonder, Will this get worse, and how quickly? Recent cohort studies (2024) show that a mild leak often stays stable for years, especially when blood pressure is wellcontrolled. However, uncontrolled hypertension, atrial fibrillation, or a history of rheumatic fever can accelerate progression, sometimes moving from grade2 to grade3 in just a few months.
When do doctors say treatment is needed?
Its not just the numbers on an echo that trigger intervention. Watch for symptoms like:
- Shortness of breath during everyday activities
- Persistent fatigue despite rest
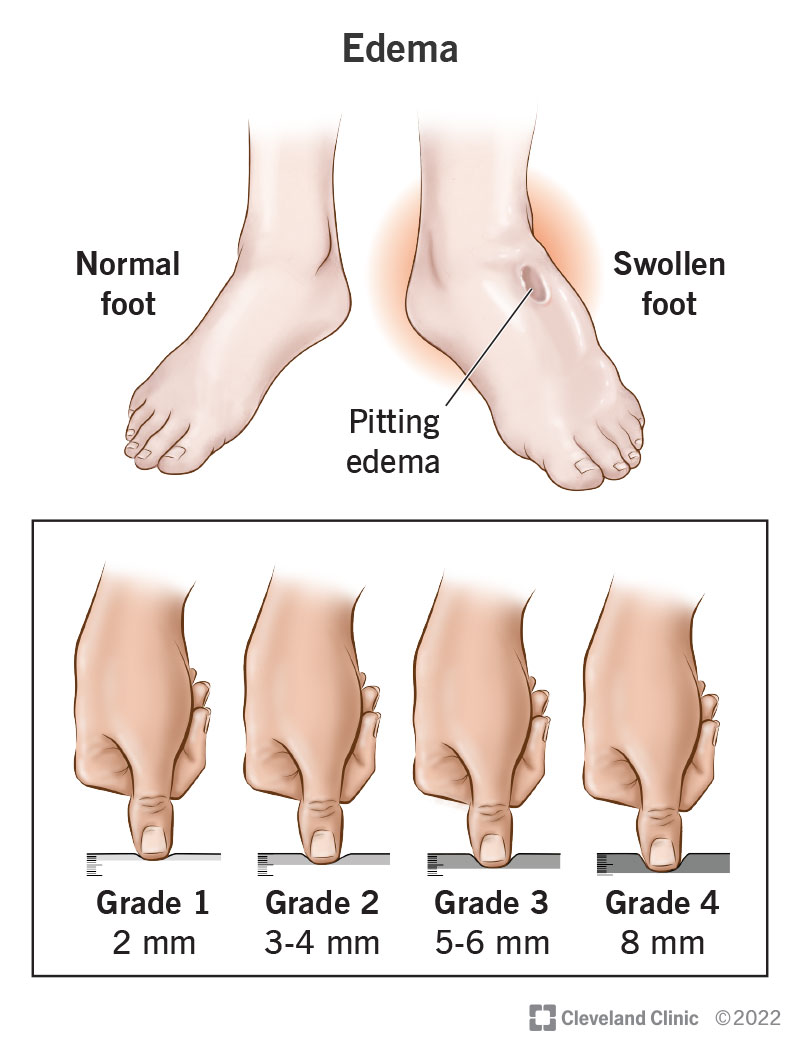
- Swelling in the ankles or abdomen
- Palpitations or irregular heartbeats
When one or more of these appear, or when imaging shows a regurgitant volume>30ml/beat, most cardiologists start talking about treatment options.
Treatment Options Overview
Medicationfirst approach (mild regurgitation)
For many with grade12 leaks, medication and lifestyle tweaks are enough. Betablockers and ACEinhibitors can lower the hearts workload, while careful salt restriction and regular aerobic exercise help keep blood pressure in check. A simple checklist can guide you:
- Are you on a betablocker or ACEinhibitor?
- Do you limit sodium to under 2,300mg per day?
- Is your weekly activity at least 150 minutes of moderate exercise?
If you check all the boxes, a watchful waiting plan may be all you need.
When surgery becomes the goto (moderatetosevere)
Once the leak reaches grade34, the heart isnt happy staying that way. Surgical repair or replacement steps in to give the valve a proper seal. Repair preserves the native valve and usually offers better longterm outcomes, while replacement (with a mechanical or bioprosthetic valve) is chosen when the tissue is too damaged.
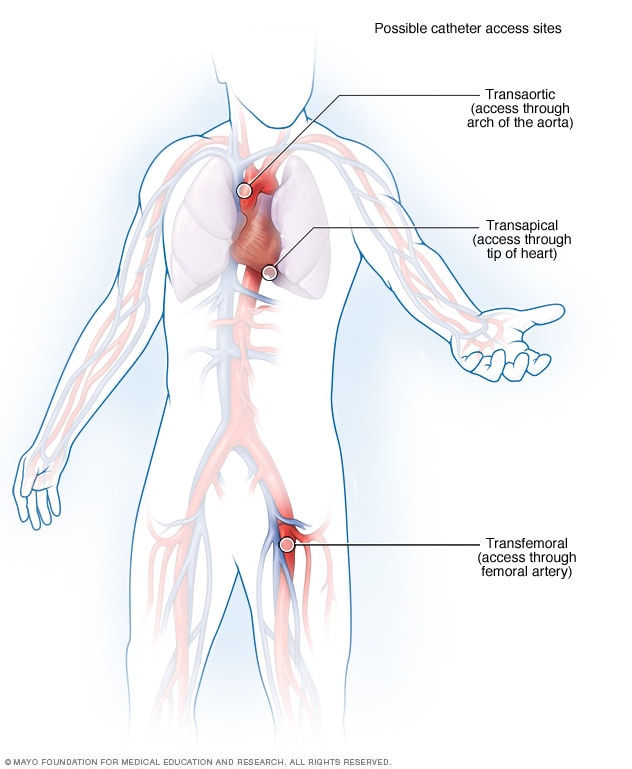
Percutaneous (catheterbased) options the noknife alternatives
Not everyone wants (or can tolerate) openheart surgery. In the past few years, catheterbased procedures have become a gamechanger.
- MitraClip: An edgetoedge repair that clips the leaking leaflets together. Ideal for patients who are older or have other health issues.
- Transcatheter mitral valve replacement (TMVR): A newer technique where a whole valve is delivered via a catheter. Early data (20242025) show promising durability.
Comparison of treatment modalities
| Option | Typical Candidates | Success Rate | Recovery Time | Durability |
|---|---|---|---|---|
| Surgical Repair | Age<75, good anatomy | 9095% | 35days hospital | 1015years+ |
| Surgical Replacement | Severe valve damage | 8590% | 710days hospital | 1020years (bioprosthetic) |
| MitraClip | High surgical risk, moderatesevere MR | 8085% | 12days hospital | 57years (still studied) |
| TMVR | Selected highrisk patients | 7580% | 23days hospital | Early data, promising |
Treatment without surgery is it possible?
Absolutely. Many patients with mild regurgitation live symptomfree for years on medication and routine monitoring. A 62yearold patient from the Mayo Clinic shared that a watchful waiting approach kept her active, hiking, and playing with grandchildren for more than five years before she needed any procedure.
Risks, Benefits & Expectations
Benefits of treating the leak
When the valve is fixedwhether by clip, surgery, or medicationyoull likely notice:
- Better exercise tolerance (no more getting wind climbing stairs)
- Reduced pressure in the lungs, meaning less nighttime coughing
- Potentially longer life expectancystudies show a median survival boost of 57years after successful repair.
Potential risks & complications
No medical decision is without risk. Heres a realistic look:
- Surgical mortality: Approximately 0.52% for repair, 25% for replacement.
- Devicerelated issues: With MitraClip, rare problems like leaflet detachment can happen, sometimes requiring another procedure.
- Infection or bleeding: As with any heart procedure, theres a small chance of infection or blood loss.
Recovery timelines & rehab tips
Recovery varies by treatment:
- Repair: Most patients leave the hospital after 35days and feel normal within 46weeks.
- Replacement: Hospital stays are longer (710days) and full activity may take 812weeks.
- MitraClip/TMVR: Hospital discharge can be as early as the next day, with light activity resumed in a week.
Cardiac rehab programsespecially those that combine gentle aerobic work with strength traininggreatly speed up the healing process. Think of it as a training camp for your heart. If you are also tracking symptoms like swelling, resources on heart failure edema and its management can be helpful alongside rehab to reduce fluid-related symptoms.
Impact on life expectancy
According to a 2024 ACC outcomes registry, patients who received a successful mitral valve repair lived on average 57years longer than those who remained untreated with moderatesevere regurgitation. Even for those managed medically, keeping blood pressure under control and staying active adds valuable years.
Practical Next Steps
Selfassessment checklist (downloadable PDF)
Before you book that next appointment, take a few minutes to run through this quick selfcheck:
- Do you feel unusually short of breath during routine chores?
- Have you noticed swelling in your legs or abdomen?
- Is your blood pressure consistently above 130/80mmHg?
- When was your last echocardiogram?
If you answered yes to any of the above, its a sign that a conversation with your cardiology team is overdue.
Preparing for your cardiology appointment
Walk into the office with confidence. Heres a short cheat sheet of questions you might ask:
- Based on my echo, am I a candidate for MitraClip or should we consider surgery?
- What are the short and longterm risks specific to my age and health profile?
- How often should I have followup imaging?
- Will my insurance cover a catheterbased procedure?
Finding a specialist you can trust
Choosing the right heart team matters. Look for cardiologists who are boardcertified and have published research on mitral valve disease. Institutions such as and the page list centers with high procedural success rates.
Financial & insurance considerations
Procedures like MitraClip can be pricey, but many insurers treat them the same as surgical repair. Ask your providers billing department about priorauthorization forms and whether there are patientassistance programs availableespecially for newer devices.
Takeaway actions
1. Review your latest echo and note the grade of regurgitation.
2. Keep a symptom diary for at least two weeks.
3. Schedule a heartteam consult and bring these questions.
4. Consider lifestyle tweaks (salt, exercise, blood pressure control) right away.
Conclusion
Mitral valve regurgitation isnt a onesizefitsall diagnosis, and the treatments range from simple medication to stateoftheart catheter procedures. By understanding the severity of your leak, recognizing symptoms early, and partnering with a trusted cardiology team, you can choose the path that best balances benefits and risks. Remember, many people live full, active lives after a successful repair or even with a wellmanaged mild leak. So, take the first step: download the selfassessment, talk to your doctor, and empower yourself with the knowledge that will keep your heart humming along for years to come.
FAQs
What are the common treatment options for mitral valve regurgitation?
Treatment ranges from medication and lifestyle changes for mild cases to surgical repair or replacement for moderate to severe cases. Minimally invasive catheter-based procedures like MitraClip and TMVR are also options for some patients.
When is surgery recommended for mitral valve regurgitation?
Surgery is usually recommended when the regurgitation is moderate to severe (grade 3-4), symptoms develop, or when the heart function is affected. Repair is preferred when feasible, but replacement is considered if valve damage is extensive.
What are the risks associated with mitral valve repair surgery?
Risks include surgical mortality (approximately 0.5% for repair), infection, bleeding, and in some cases the need for reoperation. Minimally invasive approaches may reduce recovery times and complications.
Can mitral valve regurgitation be treated without surgery?
Yes, mild mitral regurgitation can often be managed with medications such as beta-blockers and ACE inhibitors, along with lifestyle modifications and routine monitoring.
How soon can patients recover after minimally invasive mitral valve procedures?
Patients undergoing minimally invasive procedures like MitraClip or TMVR can often be discharged within 1-3 days and return to light activities within a week, while surgical repair may require a longer hospital stay and several weeks of recovery.