What Is Lateral Hip Pain
Imagine youre lying on your side, trying to drift off to sleep, and a sharp ache on the outer part of your hip keeps pulling you back into consciousness. That nagging, uncomfortable feeling is what most people refer to as lateral hip pain. Its not just a random acheits a signal from your body that something needs attention. Understanding whats behind that pain can save you weeks (or even months) of frustration, unnecessary tests, and wasted time.
In a nutshell, lateral hip pain can stem from muscles, tendons, bursae, or even the hip joint itself. The good news? Most of the time, we can pinpoint the cause with a focused history, a few simple moves, and the right imaging when needed. Lets dive straight into the most common culprits and how you can differentiate them.
Common Causes
Greater Trochanteric Pain Syndrome (GTPS)
GTPS tops the list. Its a blend of gluteus medius/minimus tendinopathy, trochanteric bursitis, and sometimes tiny tears. The pain usually sits right over the greater trochanter (the bony bump you can feel on the side of your hip) and worsens when you lie on that side, climb stairs, or stand for long periods.
Iliotibial Band Syndrome & Snapping Hip
The iliotibial (IT) band runs from your hip to the outside of your knee. When it gets tight or irritated, you may hear a snap and feel a burning sensation on the outer hip. Athletesespecially runnersrun into this one a lot.
Hip Joint Referral
Sometimes the pain isnt coming from the surface at all. Early osteoarthritis, a labral tear, or even a small fracture can radiate outward, mimicking a lateral problem. Thats why a thorough evaluation is essential.
Systematic Evaluation
History Checklist
Start with the basics:
- When did the pain start?
- Any recent trauma or increase in activity?
- Does lying on the affected side make it worse?
- Is the pain sharp, dull, burning, or throbbing?
- Any night pain that wakes you up?
PhysicalExam Moves
These maneuvers help you zone in on the source:
- Trendelenburg test: Stand on the painful leg; a dip of the opposite pelvis suggests gluteus medius weakness.
- Resisted hip abduction: Press the leg outward against resistance; pain here points toward GTPS.
- FABER (Patrick) test: Flex, abduct, and externally rotate the leg; pain in the groin hints at intraarticular issues.
- Obers test: Stretch the IT band; a tight band reproduces lateral hip discomfort.
When to Add Special Tests
If the basic moves dont give a clear answer, consider:
- Palpation of the greater trochanter for tenderness.
- Dynamic ultrasound to see tendon movement in realtime.
- Diagnostic injectioninjecting a local anesthetic into the trochanteric bursa can confirm GTPS if pain instantly eases.
Full Differential List
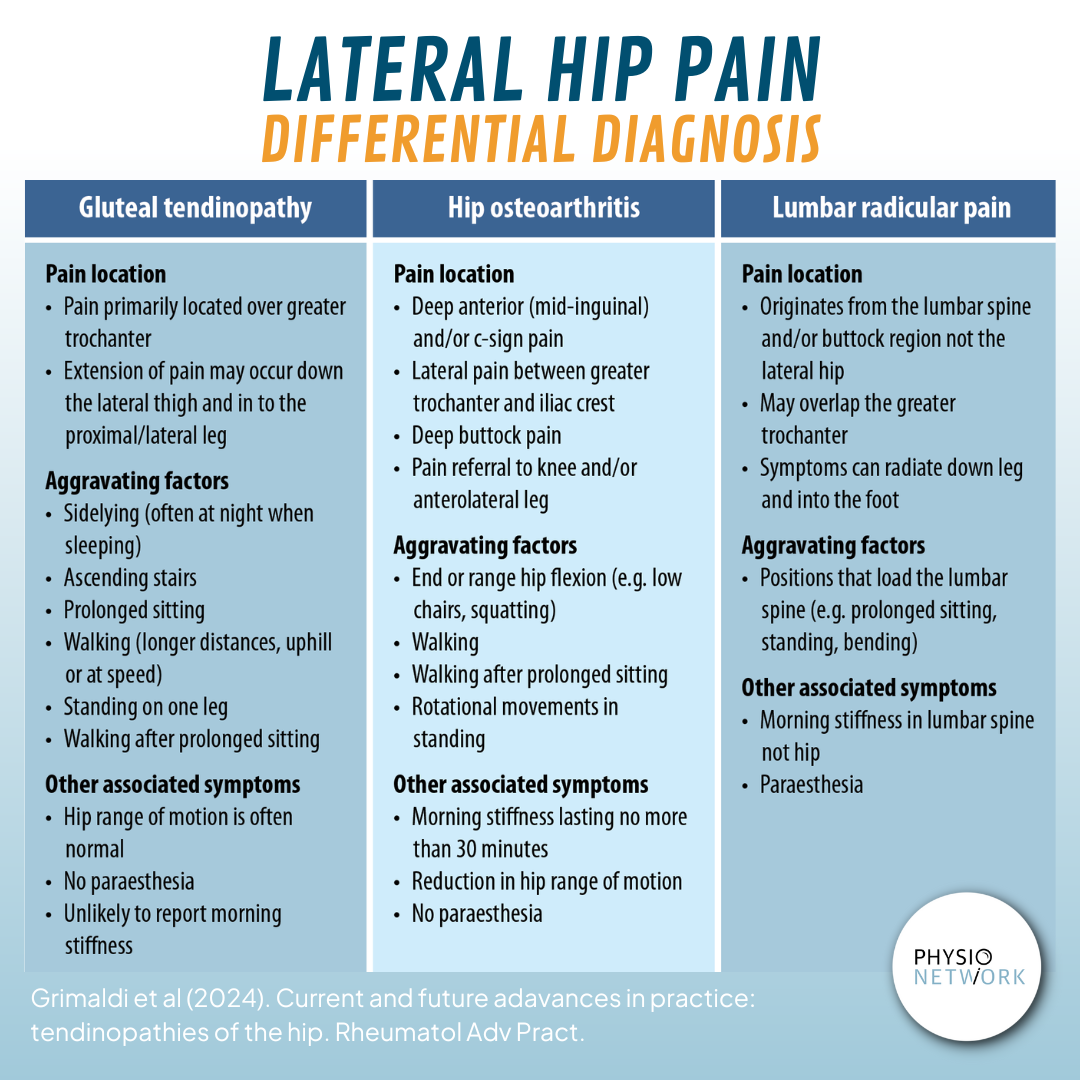
Below is a quickreference chart that separates the most common extraarticular problems from intraarticular ones. Feel free to print it out or save it as a for easy reference.
| Condition | Typical Location | Key Exam Findings | Preferred Imaging |
|---|---|---|---|
| Greater Trochanteric Pain Syndrome | Outer hip over greater trochanter | Tenderness on palpation, pain on resisted abduction | Ultrasound or MRI |
| Iliotibial Band Syndrome | Lateral thigh to hip | Positive Obers test, snapping sensation | Clinical diagnosis; MRI if persistent |
| Trochanteric Bursitis | Above greater trochanter | Local swelling, pain worsened by lying on side | Ultrasound |
| Hip Osteoarthritis | Joint space | Reduced range of motion, night pain | Xray |
| Labral Tear | Acetabular rim | Clicking, groin pain, FABER positive | MRI arthrography |
| Hip Pointer (contusion) | Greater trochanter or iliac crest | History of direct blow, localized tenderness | Xray if fracture suspected |
| Meralgia Paresthetica | Upper lateral thigh | Numbness/tingling, aggravated by tight clothing | Clinical |
| Sacroiliac Joint Dysfunction | Posterior pelvis | Pain on FABER, standing on one leg | CT or MRI if needed |
Anterior vs Posterior
FrontSide Pain
When the discomfort sits more toward the front of the hip, think about:
- Hip flexor tendinopathy (often from prolonged sitting).
- Inguinal herniaespecially if you notice a bulge.
- Acetabular labral tearpain radiates to the groin.
BackSide Pain
Posterior hip aches often involve:
- Piriformis syndrometight piriformis compresses the sciatic nerve.
- Sacroiliac joint dysfunctionpain can travel down the backside of the thigh.
- Gluteus maximus straincommon after heavy lifting.
Knowing whether the pain is more anterior or posterior helps you cut down the list of possibilities, saving time and avoiding unnecessary scans.
Imaging & Tests
Plain XRay
First line when you suspect a fracture, arthritis, or structural abnormality. Its quick, cheap, and gives a solid overview of bone health.
Ultrasound & MRI
Softtissue problems like GTPS, ITband irritation, or a small tendon tear show up best on an MRI. Ultrasound is great for guiding injections and visualizing tendon movement in real time.
Diagnostic Injections
Injecting a local anesthetic into the trochanteric bursa can be both therapeutic and diagnostic: if the pain disappears for a few hours, youve likely nailed GTPS.
Treatment Pathways
FirstLine Care
Most lateral hip issues improve with conservative measures:
- Activity modificationavoid aggravating movements.
- NSAIDs for pain and inflammation (as directed by a clinician).
- Ice packs for 1520 minutes, 34 times a day during flareups.
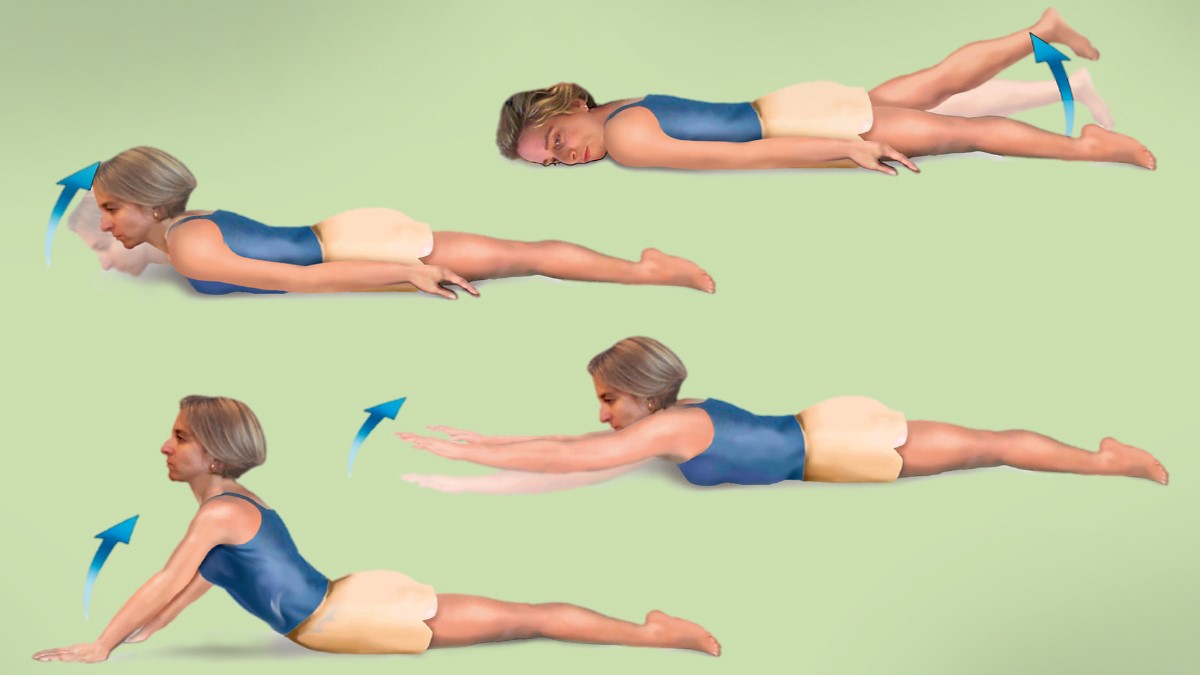
Targeted Exercises
Strengthening the gluteus medius and improving hip stability are the cornerstones of recovery. Heres a quick starter set you can do at home:
- Clamshells: Lie on your side, knees bent, lift the top knee while keeping feet together.
- Sidelying hip abduction: Keep the leg straight, raise it toward the ceiling.
- Banded walks: Place a resistance band around the thighs and step sideways.
For a printable version, download the . It includes detailed pictures and progression tips.
Physiotherapy Modalities
Beyond exercises, physiotherapists may use:
- Dry needling to release trigger points.
- Extracorporeal shockwave therapy for chronic tendinopathy.
- Manual therapy to improve hip capsule mobility.
Surgical Options
When conservative care fails after 36 months, surgery can be considered:
- Gluteus medius repairespecially for complete tendon tears.
- Bursectomyremoving inflamed bursal tissue.
- Hip arthroscopyaddressing labral tears or intraarticular pathology.
Clinical Algorithm
To keep things simple, think of the diagnostic journey as a flowchart:
- Patient presents with lateral hip pain.
- History & basic exam: Identify red flags (severe trauma, fever, night pain).
- Perform targeted maneuvers: Trendelenburg, resisted abduction, Obers test.
- If findings point to GTPS: Start conservative care + exercises.
- If red flags or unclear diagnosis: Order Xray MRI or ultrasound.
- Response to treatment?
- Improvement Continue rehab.
- No improvement Consider diagnostic injection or referral to orthopaedic specialist.
Feel free to sketch this out on a piece of paper or save a for quick reference during appointments.
Conclusion
Lateral hip pain doesnt have to be a mystery. By recognizing the hallmark signs of the most common conditionsespecially Greater Trochanteric Pain Syndromeand following a stepbystep evaluation, you can often get relief without invasive procedures. Remember, a balanced approach that combines proper history, focused physical tests, and the right imaging when needed will keep you on the fast track to recovery.
Start with the simple home exercises, keep track of what activities flare the pain, and dont hesitate to reach out to a qualified clinician if you notice any redflag symptoms. Download the for a handy visual guide, and feel free to share your story in the commentsyour experience might just help someone else on the same path.
If you have coexisting spine-related symptoms such as chronic spine inflammation, mention this to your clinician spinal pathology can sometimes refer pain to the lateral hip and change the diagnostic and treatment approach.
FAQs
What are the most common causes of lateral hip pain?
The leading culprits include Greater Trochanteric Pain Syndrome (GTPS), Iliotibial Band Syndrome, trochanteric bursitis, early hip osteoarthritis, and labral tears.
How can I differentiate GTPS from IT‑Band Syndrome on exam?
GTPS typically shows tenderness over the greater trochanter and pain with resisted hip abduction, whereas IT‑Band Syndrome often reproduces pain with Ober’s test and may produce a palpable “snap” as the band moves over the trochanter.
When is imaging necessary for lateral hip pain?
Order X‑ray if you suspect fracture, arthritis, or structural abnormality. Use ultrasound for bursitis or to guide injections, and MRI when soft‑tissue pathology (tendinopathy, labral tear) or intra‑articular disease is in doubt.
What conservative treatments work best for lateral hip pain?
Activity modification, NSAIDs, ice, and a targeted rehab program focusing on gluteus medius strengthening (clamshells, side‑lying abduction, banded walks) are first‑line. Add manual therapy, dry needling, or shock‑wave therapy if needed.
When should I consider surgical intervention?
Surgery is considered after 3–6 months of optimized conservative care without significant improvement, especially for complete gluteus medius tendon tears, refractory bursitis, or intra‑articular pathology diagnosed on MRI.