Quick answer: The 2000 tells us that if a patient fails two wellchosen antiepileptic drugs (AEDs), only about4% will become seizurefree without additional intervention. In other words, two treatment failures is the red flag that the epilepsy may be drugresistant, and its time to consider other options.
Bottom line: Look for early warning signs, act fast, and dont feel alonethere are clear steps you can take, and a lot of experts (including the original researchers) have mapped the road for you.
Landmark Study Overview
Who are Kwan and Brodie?
Philip Kwan and Ruth Brodie are neurologists who spent decades studying why some peoples seizures just wont quit, even after trying several medicines. Their work is the gold standard in epilepsy research, cited in textbooks, conference talks, and countless clinical guidelines. If you search for kwan and brodie epilepsy, youll see their names pop up everywhereproof theyre the goto authorities on drugresistant epilepsy.
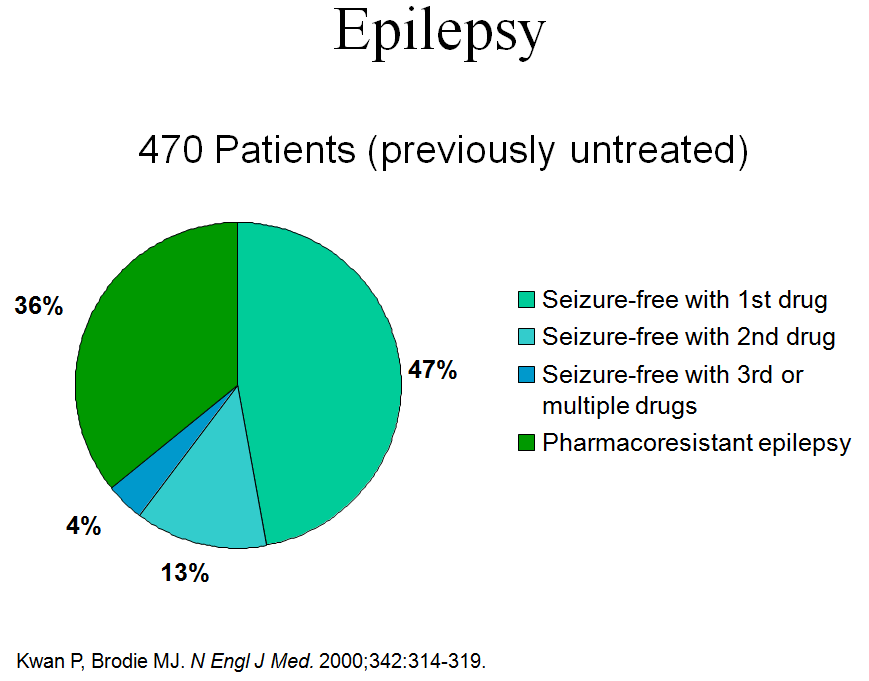
Core Findings of the 2000 NEJM Paper
The paper, often shortened to Kwan & Brodie 2000, examined over 1,500 newly diagnosed patients. The headline result? After two AED failures, roughly 4% of patients achieve seizure freedom without further changes. Thats the infamous 4percent rule. The study also identified a handful of predictors that tip the odds toward refractoriness:
- Frequent seizures before treatment (3 per month)
- Abnormal interictal EEG patterns
- Visible lesions on MRI
- Failure of the first AED due to lack of efficacy rather than sideeffects
Seeing any of these early on should make you and your doctor sit up a little straighter. The studys impact has endured for more than two decades, and it still informs the way neurologists decide when to switch strategies.
Key Statistics from Kwan & Brodie 2000
| Predictor | Odds Ratio | Clinical Takeaway |
|---|---|---|
| 3 seizures/month before treatment | 2.8 | Watch closely; consider early imaging. |
| Abnormal MRI | 2.2 | Early MRI can change the treatment plan. |
| Failure of first AED | 3.1 | Dont linger on one drug that isnt working. |
Defining Refractory Epilepsy
Official Definition
The International League Against Epilepsy (ILAE) defines refractory (or drugresistant) epilepsy as failure of adequate trials of two tolerated, appropriately chosen AED regimens to achieve sustained seizure freedom. In plain English, if two different medicinespicked for the right reasons and taken correctlydont stop the seizures, the epilepsy is considered refractory.
For a more everyday phrasing, see . Fisher emphasizes that the definition hinges on adequate trials and tolerated, meaning sideeffects matter just as much as seizure counts.
Refractory vs. HardtoControl
People sometimes use hardtocontrol when theyre not sure whether the formal criteria have been met. The distinction is subtle but important: hardtocontrol can describe any situation where seizures are frequent, while refractory is a diagnosis that triggers specific treatment pathways (e.g., surgery, neuromodulation, clinical trials).
Quick Reference Box
Refractory epilepsy = failure of 2 wellchosen AEDs
Drugresistant epilepsy (Kwan) same concept, older terminology.
Early Warning Signs
Clinical Red Flags (first 6months)
When youre newly diagnosed, keep an eye out for these signals. Theyre the early warning lights that the epilepsy might be heading toward refractoriness:
- More than three seizures a month before any medication.
- Any episode of status epilepticus (a seizure that lasts longer than five minutes).
- Focal EEG spikes that appear consistently on the same side of the brain.
- Visible structural lesions on MRI (tumors, cortical dysplasia, hippocampal sclerosis).
Lab & Imaging Clues
Beyond the bedside exam, a few tests can help confirm the risk:
- Serum drug levels: Ensuring the AED is actually reaching therapeutic concentrations.
- Genetic panels: Certain gene mutations (e.g., SCN1A) are linked to resistance.
- PET/SPECT scans: Show areas of abnormal brain metabolism that may predict poor drug response.
Checklist Is My Patient Heading Toward Refractory Epilepsy?
- 3 seizures/mo before treatment.
- Abnormal interictal EEG.
- Lesion >1cm on MRI.
- First AED stopped for lack of efficacy.
If you tick more than one box, its time to discuss a proactive plan with your neurologist. The good news? Early identification means you can move to the next step before two AED failures lock you into the refractory label.
After First AED Fails
Switch or AddOn?
The literature (including the original Kwan & Brodie cohort) shows that a simple switch to a drug with a different mechanism often yields better results than stacking another AED on top of a failing one. Why? Different mechanisms target different pathways in the brain, giving a fresh chance to break the seizure cycle.
That said, there are scenarios where an addon makes senseespecially if the first drug is welltolerated and only partially effective. The key is to make the decision based on the patients seizure type, sideeffect profile, and any comorbidities.
StepbyStep Management Algorithm
Heres a practical roadmap you can visualize (or draw on a whiteboard) when the first AED doesnt do the trick:
Algorithm Description
- Confirm adherence & therapeutic drug level: Sometimes the problem isnt the drug; its missed doses or subtherapeutic blood levels.
- Switch to a second AED with a different mechanism: For example, move from a sodium channel blocker (like carbamazepine) to a GABAenhancer (like valproate).
- If seizures persist after the second trial, consider early referral: Options include epilepsy surgery, vagus nerve stimulation, responsive neurostimulation, or enrollment in clinical trials.
- Engage a multidisciplinary team: Neurologist, neuropsychologist, epilepsy nurse, and social worker can address the medical, cognitive, and psychosocial aspects.
Remember, the goal isnt just to stop seizures; its to improve quality of life, keep you independent, and reduce the emotional toll that uncontrolled epilepsy can bring.
Real World Stories
Case Study: A Young Adult Finds a New Path
Meet Alex, a 23yearold college student who was diagnosed with focal epilepsy at 16. After the first AED (lamotrigine) failed, Alexs neurologist followed the Kwan & Brodie approach: confirm drug levels, switch to levetiracetam, and order an MRI. The scan revealed a subtle cortical dysplasia. Because the redflag checklist was positive, Alex was referred to a epilepsy surgery center after the second AED also fell short. He eventually underwent a focal resection, and three years later hes seizurefree and back in the classroom.
Alexs story illustrates three important lessons:
- Early identification of risk factors speeds up referral.
- Imaging can uncover treatable structural causes.
- Surgery is a viable, often lifechanging option for refractory cases.
Oldest Living Person with Epilepsy A Testament to Resilience
Gertrude, now 102, holds the title of the oldest living person with epilepsy. She was diagnosed in the 1940s, long before modern AEDs existed. Her secret? A supportive family, meticulous pill schedules, and a lifelong habit of keeping a seizure diary. While she never needed surgery, her case reminds us that epilepsy isnt a deadline disease; with the right care, people can thrive for decades.
Life With Epilepsy: 50 Facts Snapshot
Here are a handful of quick, bitesize facts (drawn from the life with epilepsy 50 facts resource) that can empower you:
- About 1% of the worlds population lives with epilepsy.
- Twothirds of patients become seizurefree with the right drug regimen.
- Only 30% of those who are drugresistant qualify for surgery, but surgery can achieve seizure freedom in up to 70% of suitable candidates.
- Stress, sleep deprivation, and alcohol are common seizure triggers.
- Driving restrictions vary, but many jurisdictions allow driving after a seizurefree period of 6months.
These facts reinforce that while epilepsy can be daunting, knowledge, early action, and a solid support network make a world of difference.
Conclusion
Whether youre a newly diagnosed patient, a family member, or just someone curious about kwan and brodie epilepsy, the takeaway is clear: two AED failures signal a need for a new strategy, and the early signs are often visible if you know what to look for. By using the redflag checklist, confirming drug levels, and acting on imaging findings, you can move from the uncertainty of hardtocontrol to a proactive planwhether thats a different medication, a surgical option, or a clinical trial.
Take the next step today: download the free casestudy PDF, talk to your neurologist about the 4percent rule, and remember youre not alone on this journey. If you have questions, feel free to reach outour community is here to help you navigate the path toward seizure freedom. For patients needing support navigating insurance and access to costly therapies, resources like Exondys 51 insurance can provide guidance on coverage options and financial assistance.
FAQs
What is the main finding of the Kwan and Brodie epilepsy study?
The study found that if a patient fails treatment with two well-chosen antiepileptic drugs (AEDs), only about 4% are likely to achieve seizure freedom without further intervention, marking two AED failures as a key indicator of drug-resistant epilepsy.
How is refractory epilepsy defined according to Kwan and Brodie?
Refractory epilepsy is defined as the failure of adequate trials of two tolerated and appropriately chosen AED regimens to achieve sustained seizure freedom.
What are early warning signs of refractory epilepsy?
Warning signs include having more than three seizures per month before treatment, abnormal EEG patterns, visible structural lesions on MRI, and failure of the first AED due to lack of efficacy rather than side effects.
What should be the clinical approach after the first AED fails?
Confirm drug adherence and therapeutic levels, then switch to a second AED with a different mechanism of action. If seizures persist after two AED trials, consider referral for epilepsy surgery, neuromodulation, or clinical trials.
Why is early identification of drug-resistant epilepsy important?
Early identification allows for timely changes in treatment strategy, including consideration of surgery or alternative therapies, which can improve seizure control and quality of life before labeling epilepsy as refractory.