Well unpack the most common safety concerns, compare the bestandsafest medications, and even give you a cheatsheet for a conversation with your doctor. By the end, youll know exactly which drugs to watch out for, which ones can be a reasonable choice, and how lifestyle tweaks can become your secret weapon against osteoporosis.
Medication Landscape
What Are the Most Prescribed Osteoporosis Drugs?
In the United States and many western countries the mostprescribed options fall into three families:
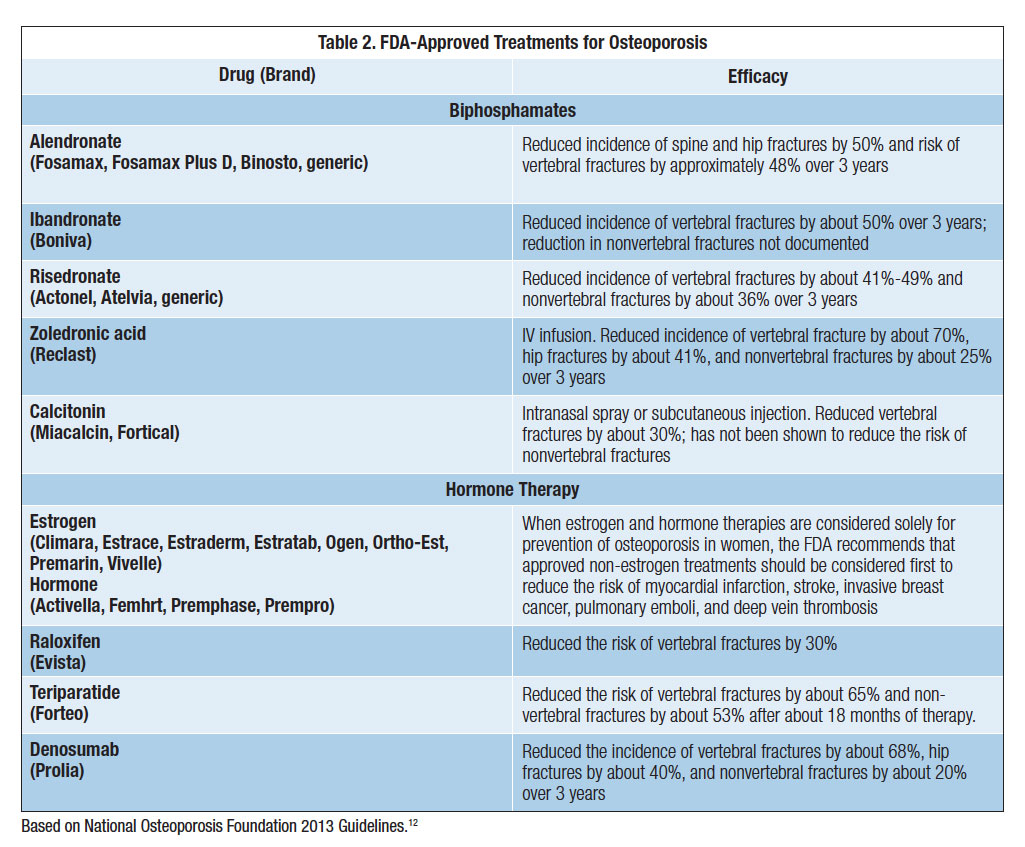
- Bisphosphonates alendronate (Fosamax), risedronate (Actonel), ibandronate (Boniva), and the yearly IV infusion zoledronic acid (Reclast).
- Monoclonal antibodies denosumab (Prolia) given as a subcutaneous injection every six months, and romosozumab (Evenity) administered monthly.
- Selective estrogenrelated modulators (SERMs) raloxifene (Evista), which also helps with breast health.
How Do These Drugs Work?
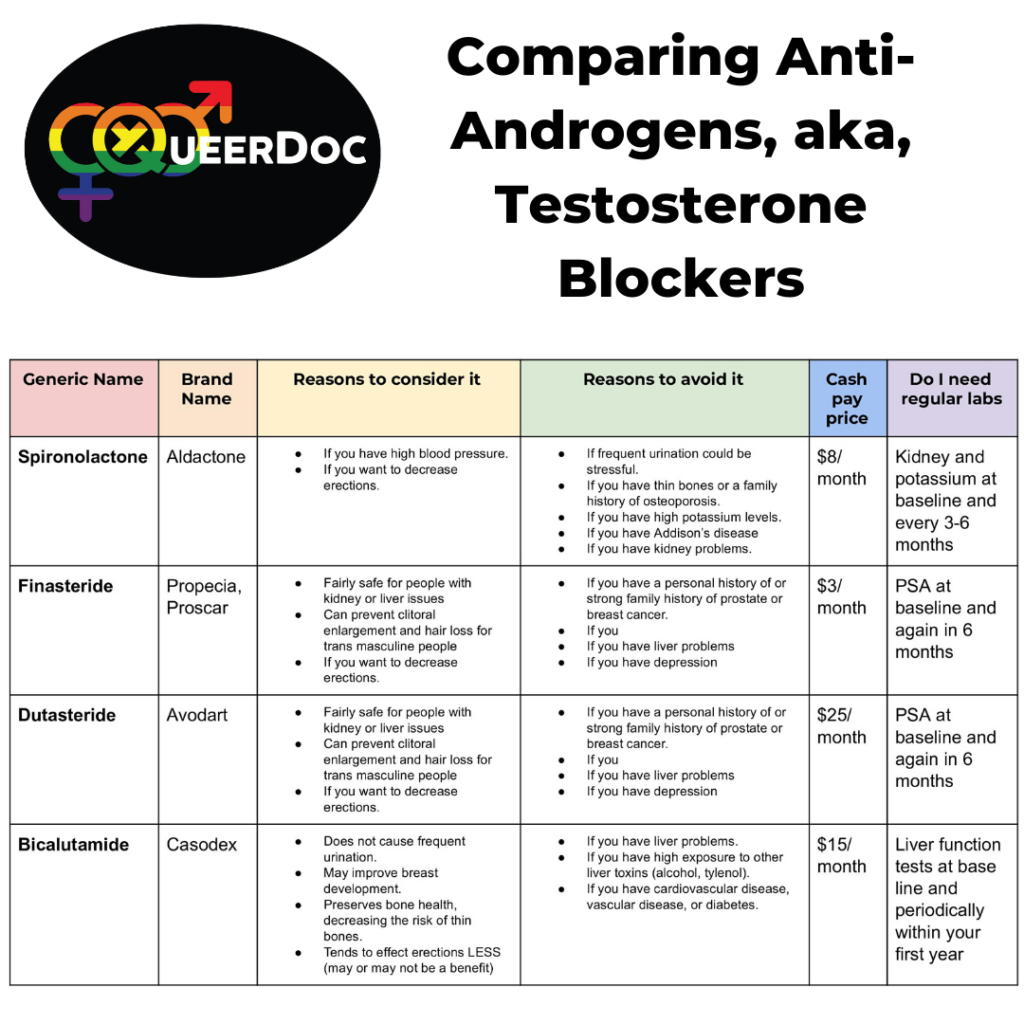
Bisphosphonates bind to bone surfaces and slow down the cells that break down bone (osteoclasts). Denosumab works a bit like a brake on the same cells, while romosozumab actually encourages new bone formation before later switching to a braking mode. SERMs are a hybrid, mimicking estrogens boneprotective effects without the hormones other risks. For readers curious about broader drug classes and mechanisms, a clear primer on how anti-androgens work illustrates how different drugs can act on specific pathways a useful comparison when thinking about targeted therapies for bone versus other conditions.
Quick Reference Table
| Drug | Class | Typical Dose | Route |
|---|---|---|---|
| Alendronate | Bisphosphonate | 70mg weekly | Oral |
| Zoledronic Acid | Bisphosphonate | 5mg yearly | IV |
| Denosumab | Monoclonal Antibody | 60mg every 6months | SubQ Injection |
| Romosozumab | Monoclonal Antibody | 210mg monthly | SubQ Injection |
| Raloxifene | SERM | 60mg daily | Oral |
Safety Concerns
Atypical Femoral Fracture (AFF)
One of the most talkedabout dangers is an odd break in the thigh bone that looks like a stress fracture. Its rareabout 1 in 1,000 patients on longterm bisphosphonatesbut it can happen after five or more years of use. The pain often starts as a dull ache that persists for weeks, and many people ignore it until the bone actually snaps.
RealWorld Example
Imagine a 68yearold woman named Helen who took alendronate for seven years. She brushed off a persistent thigh soreness, assuming it was just a muscle strain. Eventually, she felt a pop while climbing stairs and was diagnosed with an AFF. The fracture required surgery and a lengthy rehabsomething that could have been prevented with a drug holiday or earlier imaging.
Osteonecrosis of the Jaw (ONJ)
ONJ is a condition where the jawbone starts to die, often after a dental extraction. The risk is highest with highdose IV bisphosphonates and denosumab, especially in cancer patients, but even lowdose osteoporosis regimens can be a factor. Symptoms include sore gums, exposed bone, and sometimes a foul taste.
Common SideEffects That Irritate Everyday Life
- Gastrointestinal upset heartburn, esophageal irritation (especially with oral bisphosphonates).
- Muscle or joint pain can mimic arthritis.
- Elevated cholesterol observed in some users of alendronate.
- Kidney function drops a concern with IV zoledronic acid, especially if you already have renal issues.
When to Call Your Doctor Immediately
- Sudden, severe jaw pain or swelling.
- Unexplained thigh or groin ache that lasts longer than a week.
- New onset of high fever after an injection.
- Blood in the urine or sudden swelling in the ankles.
Risk Profiles
Who Is Most Vulnerable?
Age alone isnt the whole story. The biggest red flags are:
- Being over 70years old and on a bisphosphonate for more than five years.
- Having chronic kidney disease (CKD) even stage3 can raise the risk of kidney injury from IV drugs.
- History of gastrointestinal ulcers or esophageal strictures.
- Previous jaw surgery or invasive dental work without proper prophylaxis.
Personal Anecdote
Mike, 72, had a smooth run with his yearly zoledronate infusion until he needed a tooth extraction. His dentist didnt warn him about ONJ, and a few weeks later he developed a painful, nonhealing socket. After a consultation, his doctor switched him to a lowdose oral bisphosphonate with a strict dental monitoring plan.
Best & Safest Options (20232024)
Drugs With the Lowest Documented SideEffects
Based on recent metaanalyses, the lowrisk list includes:
- Lowdose weekly alendronate (70mg) still a bisphosphonate but with a wellstudied safety profile.
- Onceyearly IV zoledronate convenient and the overall risk of AFF and ONJ is lower when renal function is normal.
- Raloxifene particularly good for women who also need breastcancer risk reduction.
Balancing Benefits and Risks
If youre looking for the best and safest treatment for osteoporosis 2023, many experts recommend a personalized plan: start with a lowdose oral bisphosphonate, monitor bone density yearly, and consider a drug holiday after five years if your fracture risk has dropped. For those who cant tolerate oral pills, the yearly zoledronate infusion often wins the safetyvsconvenience battle.
Emerging Therapies With Promising Profiles
Romosozumab shows strong bonebuilding results, but early data flagged a slight increase in cardiovascular events, so its usually reserved for patients with very high fracture risk who can tolerate the price and monitoring.
Safety Score Comparison
| Drug | Safety Score (05) | Injection Frequency | Typical Cost (US$) | FDA Approval |
|---|---|---|---|---|
| Alendronate | 4 | Oral weekly | ~$30$50 | 1995 |
| Zoledronic Acid | 4.5 | IV yearly | ~$300$400 | 2005 |
| Denosumab | 3.5 | Injection q6mo | ~$1,200$1,500 | 2010 |
| Romosozumab | 3 | Injection monthly | ~$3,000$4,000 | 2019 |
| Raloxifene | 4 | Oral daily | ~$150$200 | 1997 |
DrugFree Strategies
Nutrition Basics
Calcium alone isnt enoughyou also need vitaminD (8001,000IU daily), magnesium, and vitaminK2 to direct calcium to the bones. Dairy, leafy greens, fortified plant milks, and a modest amount of fatty fish can cover most bases. If youre unsure, a short blood test can tell you if you need a supplement.
Exercise That Actually Builds Bone
Weightbearing moves (walking, hiking, dancing) and resistance training (light dumbbells, resistance bands, bodyweight squats) trigger boneforming cells. Aim for at least 30minutes of moderate activity most days, with two strength sessions per week. A simple 12week home plan might look like:
- Weeks14: 15minute brisk walk + 10minutes of wall pushups.
- Weeks58: Add 5minutes of stepups and 210 bodyweight squats.
- Weeks912: Incorporate 2310lb dumbbell rows and a 20minute jog.
Lifestyle Tweaks
Quit smoking, limit alcohol to 2 drinks per day, and keep your home free of tripping hazards (loose rugs, poor lighting). These simple changes can shave years off your fracture risk and complement any medication you decide to use.
Case Study
Laura, 65, stopped her monthly bisphosphonate after a scare about jaw pain. She committed to a calciumrich diet, vitaminD supplements, and the 12week regimen above. After nine months, her bonedensity scan showed a small but statistically significant increase in lumbar spine Tscoreproof that nondrug measures can truly make a difference.
Talking to Your Doctor
Shared DecisionMaking Checklist
Bring a printed copy of this list to your next appointment. It shows that youre engaged, informed, and ready to cocreate a plan:
- What is the safest medication for my kidney function and dental history?
- Can we schedule a drug holiday after five years, and how will we monitor bone loss?
- What lab tests (creatinine, vitaminD, calcium) should be repeated regularly?
- How often should I have a dental checkup while on therapy?
- Are there lifestyle changes that could let me lower the dose or stop medication?
Understanding Test Results
When you get your DXA scan, ask the doctor to explain the Tscore and what a 0.5point change means for you personally. A small decline doesnt always signal failure; sometimes it simply reflects natural aging.
Printable Conversation Sheet
Feel free to copy and fill in your answers before the visit. Having your thoughts written down reduces anxiety and keeps the conversation focused.
Conclusion
The dangers of osteoporosis drugs are real, but theyre also manageable when you know what to watch for and work with a knowledgeable clinician. Understanding who is most at risk, selecting a drug with a favorable safety profile, and pairing treatment with solid nutrition, exercise, and lifestyle habits gives you a balanced, empowered approach to bone health. Remember, you dont have to navigate this aloneuse the doctorvisit checklist, stay curious, and keep the conversation open. Your bones thank you for the care you invest today.
FAQs
What are the most common side‑effects of osteoporosis drugs?
Typical side‑effects include gastrointestinal irritation, muscle or joint pain, elevated cholesterol, and, for some drugs, a risk of atypical femoral fractures or jaw osteonecrosis.
How long should I stay on bisphosphonates before considering a drug holiday?
Most guidelines suggest a drug holiday after 5 years of oral bisphosphonate use or 3 years of IV therapy, provided your fracture risk has decreased and bone density remains stable.
Can I switch from denosumab to another medication safely?
Yes, but you should transition to another anti‑resorptive (like a bisphosphonate) within 6–8 weeks of the last denosumab injection to avoid rapid bone loss.
Is osteonecrosis of the jaw only a concern for cancer patients?
No. While the risk is highest with high‑dose IV therapy for cancer, even low‑dose osteoporosis regimens can cause ONJ, especially after invasive dental work without proper precautions.
What lifestyle changes can reduce my reliance on osteoporosis medications?
Focus on adequate calcium, vitamin D, and vitamin K2 intake, regular weight‑bearing and resistance exercise, smoking cessation, limiting alcohol, and maintaining a safe home environment to prevent falls.