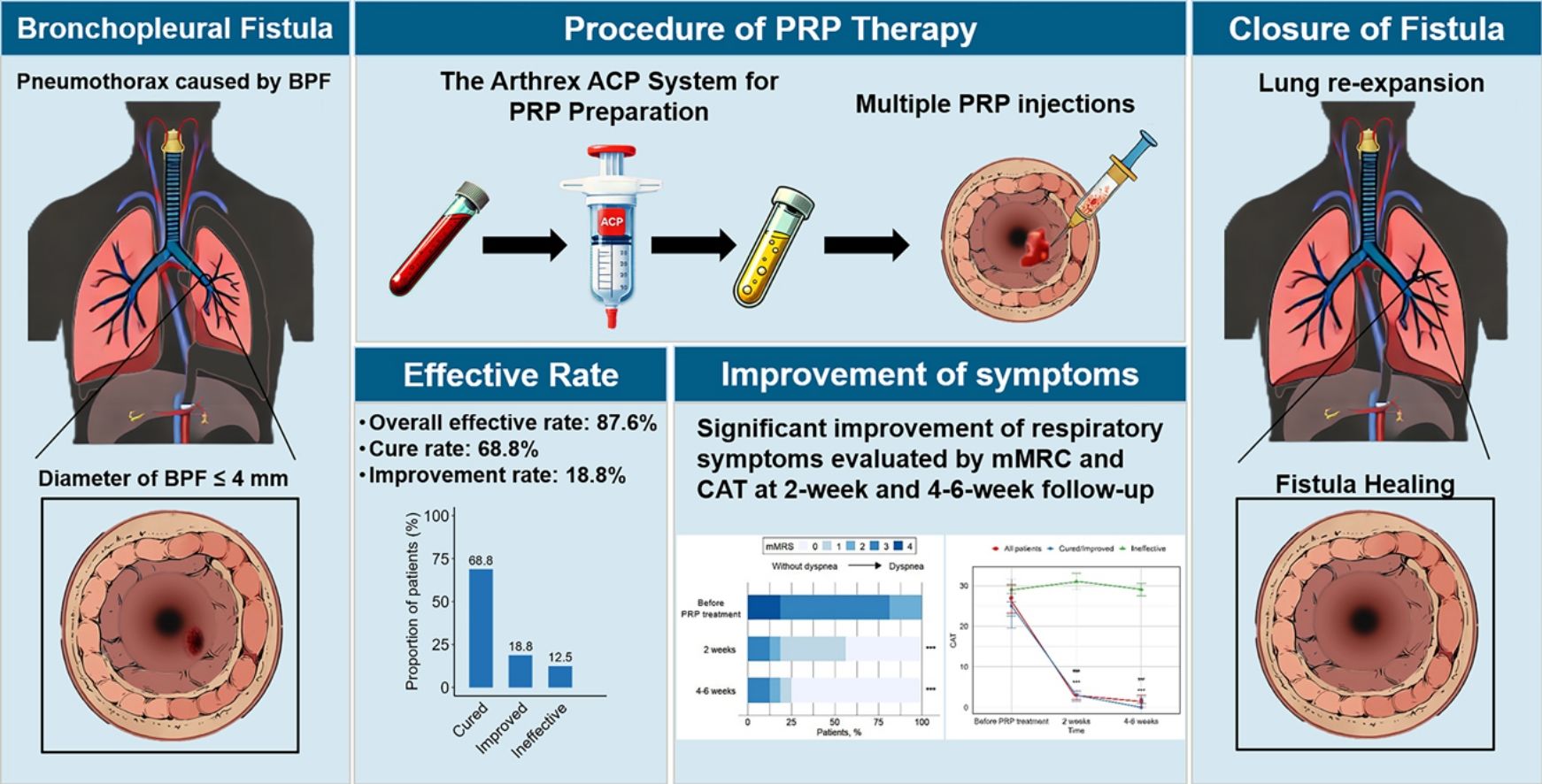
Short answer: A bronchopleural fistula (BPF) is an unwanted tunnel between a lung airway and the pleural space, most often caused by surgery, infection, or lungdestroying treatments. Knowing the exact cause helps you spot symptoms early, avoid complications, and choose the right fix whether its a chesttube tweak or a bigsurgery plan.
What Is BPF?
Bronchopleural fistula meaning
In plain language, a BPF is a hole that lets air escape from a bronchus straight into the space around the lungs (the pleural cavity). That air leak can keep your chest drain bubbling nonstop and, if untreated, can lead to serious breathing problems.
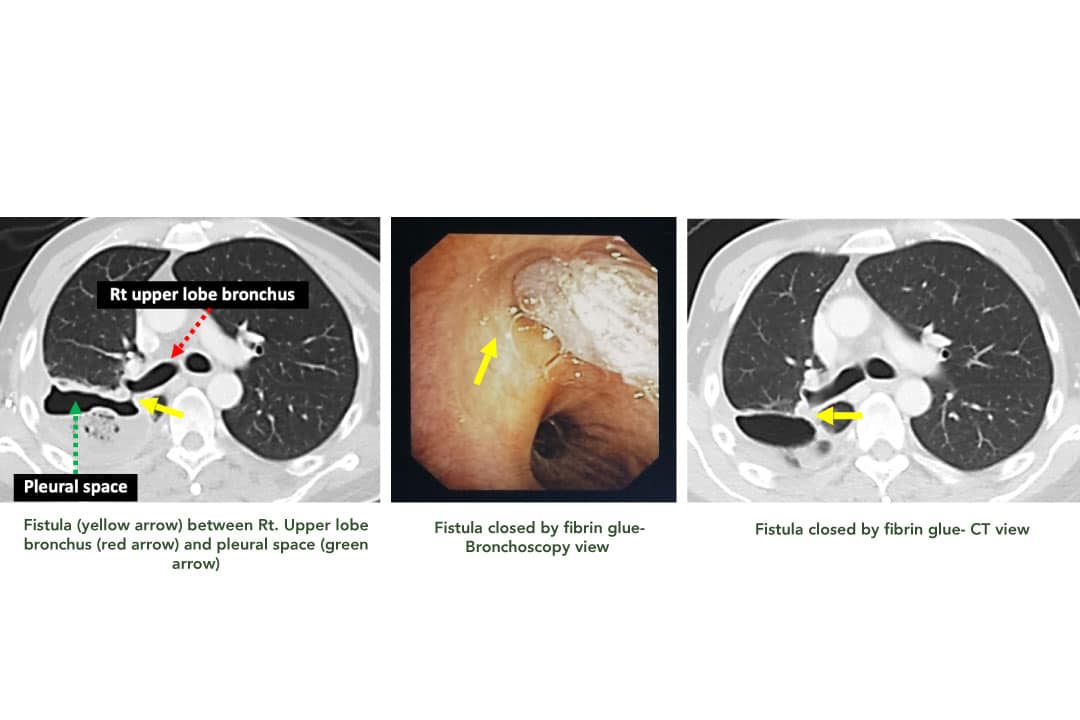
Visual aid
If you prefer a quick visual, there are several that sketch the anatomy and show where the tunnel forms.
Why it matters
Understanding the definition is the first step because every decision from imaging to surgery revolves around that tiny pathway.
Key Causes Explained
What surgical complications lead to BPF?
Most BPFs appear after lung resections such as lobectomy or pneumonectomy. The usual suspects are:
- Staple line failure a misfired stapler can leave a weak spot that tears under pressure.
- Poor bronchial suturing if the stitch isnt tight enough, air finds the path of least resistance.
- High anastomotic tension pulling too hard on the bronchial stump can cause it to pull apart.
According to a study in , postoperative BPFs show up in 15% of major lung surgeries, with higher rates after pneumonectomy.
How do infections create a fistula?
Necrotizing pneumonia, lung abscesses, and empyema can erode the bronchial wall. The infection essentially eats through tissue, creating a direct airwaypleura connection.
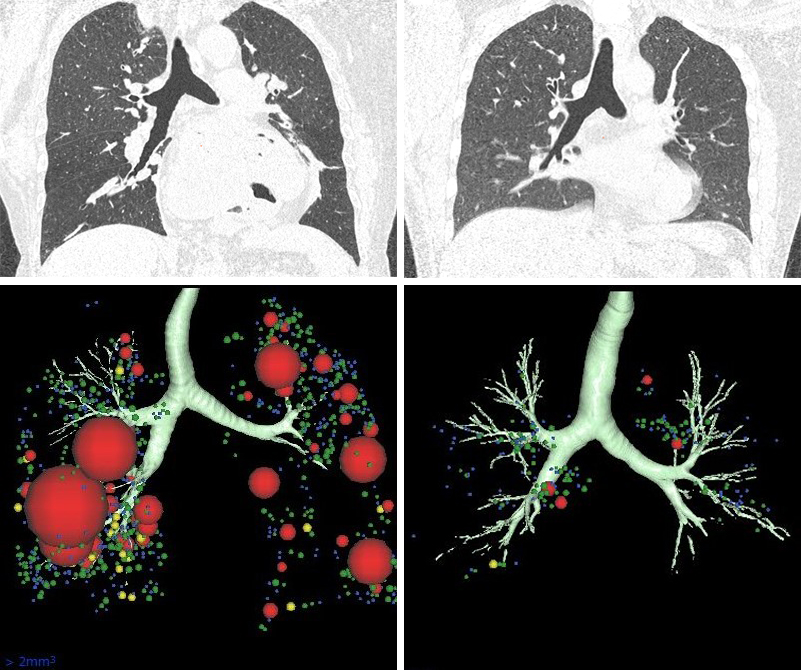
Radiology articles on illustrate how CT scans reveal airfluid levels that hint at this destructive process.
Can a spontaneous pneumothorax cause BPF?
When a large bleb bursts, the resulting pneumothorax can occasionally rupture a nearby bronchus, forming a fistula without any prior surgery.
Are chemo, radiotherapy or TB culprits?
Both chemo and radiation can cause fibrosis and necrosis of lung tissue, weakening the bronchial wall. Tuberculosis, especially reactivation in an immunocompromised patient, can also chew through the airway.
What about bronchopleural fistula after chest tube?
Yes, an improperly placed or overinflated chest tube can puncture a bronchus. Though rare, case series have reported this iatrogenic cause, especially when suction is set too high.
Any other rare triggers?
Trauma, foreignbody aspiration, and even bronchoscopyinduced perforations have been documented as unusual origins of BPF.
Realworld glimpse
Imagine a 62yearold lungcancer patient who just had a right upperlobe pneumonectomy. The surgeon notices a small air leak during closure, but decides to finish the case. Two days later, the patients chest drain bubbles nonstop, and a CT scan shows a tiny fistula. That scenario is a textbook example of postoperative BPF.
Fistula Grading Explained
Whats the grading scale?
Clinicians often use a fourgrade system based on leak size, timing, and clinical impact:
| Grade | Leak Size | Typical Timing | Management Hint |
|---|---|---|---|
| I | Mini <1mm | Immediate postop | Observation, low suction |
| II | Small 13mm | Within 7days | Chesttube adjustment, possible endobronchial valve |
| III | Moderate 35mm | 714days | Consider surgical repair or muscleflap coverage |
| IV | Large >5mm | >14days | Urgent surgery, possible ECMO support |
Why grading matters for ventilation?
Highergrade leaks often require lowpressure ventilation strategies to avoid blowing the fistula wider. Thats why guidelines emphasize permissive hypercapnia and low tidal volumes.
How to Diagnose
What clinical clues should raise suspicion?
Look for a persistent air leak (bubbling in the drainage system), sudden subcutaneous emphysema, or a newonset cough that worsens with inspiration.
Which imaging works best?
A chest Xray is the first step, but a highresolution CT scan is the gold standard for visualizing the exact tunnel. Radiology texts describe airfluid levels in the pleural space as a hallmark sign of a BPF.
Can bronchoscopy help?
Yes. A flexible bronchoscope lets doctors see the bronchial side of the fistula and even place an endobronchial valve to seal the leak temporarily.
Do labs add anything?
Analyzing pleural fluid for bacterial growth helps differentiate a simple air leak from an infected empyema, which would demand antibiotics.
Complication Risks Explained
What are the acute complications?
- Tension pneumothorax air builds up fast, pushing the lung and heart.
- Massive air leak can exhaust the ventilator and cause respiratory failure.
- Septic empyema infection spilling into the pleural cavity.
What are the chronic issues?
- Persistent empyema leading to fibrothorax.
- Bronchiectasis from repeated infections.
- Weight loss and malnutrition due to ongoing illness.
How do complications affect mortality?
Metaanalyses report 30day mortality rates up to 20% for highgrade BPFs, especially when accompanied by sepsis or severe respiratory compromise.
Patient perspective
One survivor shared, When my chest tube kept bubbling for days, I thought Id never breathe normally again. The team explained the fistula, fixed it, and Im back to hiking. Stories like this underscore why early detection matters.
Treatment Options Overview
Ventilation management
Lowtidalvolume ventilation (46mL/kg) with permissive hypercapnia reduces airway pressure, limiting further damage. If the leak persists, clinicians may switch to a waterseal system to let the fistula close on its own.
Chesttube strategies
For bronchopleural fistula after chest tube, key steps include:
- Repositioning the tube under fluoroscopy.
- Lowering suction to 1015cmHO.
- Using a smallerdiameter tube if the leak is minor.
Surgical options
When the leak is GradeIII or IV, surgeons may:
- Directly staple or suture the bronchial stump.
- Cover the area with a muscle flap (intercostal or latissimus dorsi) for extra protection.
- Perform a pneumonectomy completion if the lung segment is nonviable.
Nonsurgical adjuncts
Endobronchial valves, fibrin glue, and chemical pleurodesis are minimally invasive tools that can seal a leak while buying time for the patients condition to improve.
For targeted airway clearance and improving secretion management that can reduce infection risk after a leak, evidence-based techniques like chest physiotherapy cystic fibrosis approaches may be adapted by physiotherapists to suit non-CF postoperative patients.
Rehabilitation and followup
After the fistula is closed, pulmonary rehab helps restore lung capacity. Serial CT scans every 12months ensure the tunnel stays sealed.
Preventing BPF Risks
Preoperative measures
Smoking cessation at least 4weeks before surgery, optimizing nutrition (protein>1.2g/kg/day), and thorough preop pulmonary function testing lower the odds of a postoperative fistula.
Intraoperative techniques
Surgeons now use reinforced staplers and doublesuture reinforcement to secure the bronchial stump. Avoiding excessive tension and checking the staple line intraoperatively with bronchoscopy can catch leaks before closing the chest.
Postoperative monitoring
Early chesttube monitoring for bubbling, daily chest Xrays, and a low threshold for CT when air leaks persist are essential. A stopwatch approach measuring leak duration helps decide when to intervene.
Fast FAQ Answers
What are the most common causes of a bronchopleural fistula?
The top causes are postoperative complications after lung resection, necrotizing infections, and damage from chemoradiation or tuberculosis.
How soon after surgery does a BPF usually appear?
Most patients develop symptoms within the first two weeks after lung surgery.
Can a chest tube cause a BPF?
Yes an improperly placed or overinflated chest tube can puncture the bronchus, leading to a fistula.
What imaging best shows a BPF?
Highresolution CT scanning is the gold standard for visualizing the bronchialpleural connection.
Is there a grading system for BPF?
Yes BPFs are graded IIV based on leak size, timing, and clinical impact.
Essential Takeaway List
- Know the key causes: surgery, infection, radiation, TB, and chesttube mishaps.
- Spot early signs: persistent bubbling, subcutaneous emphysema, sudden dyspnea.
- Use CT and bronchoscopy for definitive diagnosis.
- Apply the grading system to guide treatment intensity.
- Lowpressure ventilation and proper chesttube management are firstline fixes.
- Consider endobronchial valves or surgical repair for persistent leaks.
- Preventive steps before and after surgery dramatically cut risk.
Understanding bronchopleural fistula causes isnt just academic it can be the difference between a quick recovery and a prolonged, dangerous battle with air leaks. If youve dealt with a BPF yourself or have questions about the steps above, feel free to share your experience in the comments. Together we can turn a scary medical term into something we all know how to handle.
FAQs
What are the most common causes of a bronchopleural fistula?
Post‑operative complications after lung resection, necrotizing infections, and tissue damage from chemotherapy, radiation or tuberculosis are the leading causes.
When do bronchopleural fistulas usually appear after surgery?
Most BPFs become symptomatic within the first two weeks following lung surgery, though some can present later if the leak persists.
Can a chest tube itself cause a bronchopleural fistula?
Yes—improper placement or excessive suction from a chest tube can puncture a bronchus and create a fistula, though this is rare.
Which imaging modality best visualizes a bronchopleural fistula?
A high‑resolution CT scan is the gold standard for identifying the exact bronchial‑pleural connection and any associated air‑fluid levels.
How is the severity of a bronchopleural fistula graded?
Clinicians use a four‑grade system (I‑IV) based on leak size, timing, and clinical impact; higher grades often require surgical repair and low‑pressure ventilation strategies.