If you or someone you love has just heard the words stage4 prostate cancer, your mind probably spun into a frenzy of questions, fears, and the desperate wish for a clear answer. Lets cut to the chase: the most effective firstline approach today is a combination of hormone (androgendeprivation) therapy with newer drugs such as abiraterone or enzalutamide, and when needed chemotherapy or targeted radiation. These strategies aim to shrink the tumors, keep the disease from spreading further, and extend survival while trying to preserve quality of life.
Below, Ill walk you through what stage4 really means, the core treatments that have proven most beneficial, how to personalize the plan for your unique situation, and stories that show why hope isnt lost. Think of this as a friendly chat over coffee, where Im here to listen, explain, and maybe share a laugh or two along the way.
Understanding Stage 4
What stage4 actually means
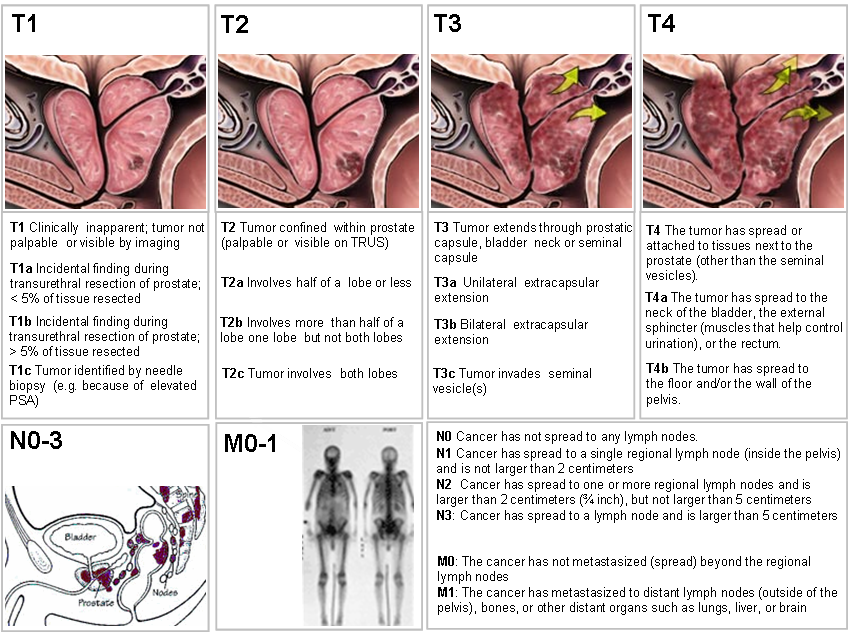
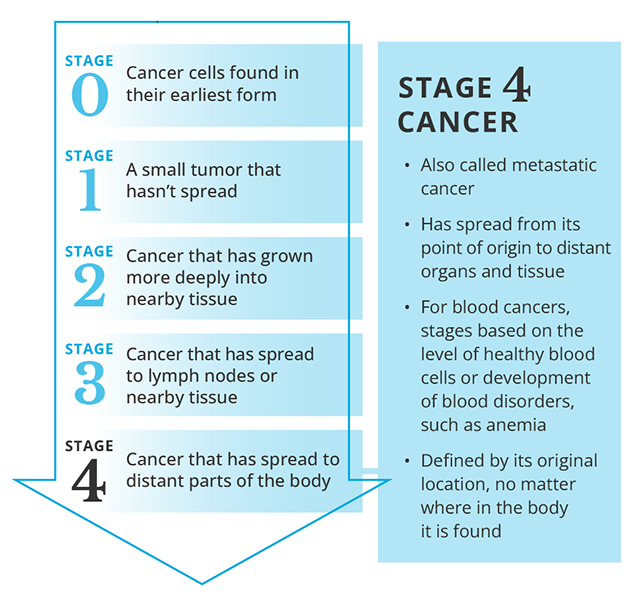
Stage4, also called metastatic prostate cancer, means the cancer has escaped the prostate and traveled to other parts of the body most often the bones, but also the lymph nodes, liver, or lungs. Its not a single uniform disease; the spread can be limited (oligometastatic) or widespread, and each pattern calls for a slightly different game plan.
How doctors diagnose it
Diagnosis typically involves a mix of blood tests (PSA levels), imaging, and sometimes biopsies. Modern imaging like PSMAPET scans can spot tiny metastases that older bone scans might miss. The Gleason score from the original prostate tissue also helps gauge how aggressive the tumor is.
Realworld example: My dad has stage4 prostate cancer
When my dad got the diagnosis, the doctor showed us a 3D map of his bone lesions. Seeing the disease visualized was unsettling, but it also gave us a concrete starting point for treatment discussions. He was 68, otherwise healthy, and his team quickly moved to start hormone therapy, which gave him a noticeable energy boost within weeks.
Survival statistics and lifeexpectancy calculators
Current data from the National Cancer Institute (NCI) and the Mayo Clinic indicate a median survival of about 35years for most men receiving modern combination therapy. Some patients, especially those with limited metastatic spread and favorable genetics, live 710years or more. Online lifeexpectancy calculators can give a ballpark figure, but theyre based on population averages your personal journey may differ. For more on prostate removal life expectancy and how treatments affect long-term outcomes, review targeted resources that compare survival after different interventions this can help set realistic expectations during planning.
Core Treatment Options
Hormone (AndrogenDeprivation) Therapy the backbone
Prostate cancer cells thrive on testosterone. By cutting off that fuel, we can stall growth. The first line usually involves LHRH agonists or antagonists (e.g., leuprolide, degarelix). Most patients start here because its effective, relatively welltolerated, and the foundation for other treatments.
Newgeneration hormonal agents
Over the past decade, drugs that go deeper into the hormonal pathway have entered the scene:
- Abiraterone (Zytiga) blocks an enzyme that helps tumors make their own testosterone. Its given with lowdose prednisone to manage sideeffects.
- Enzalutamide (Xtandi), Apalutamide (Erleada), and Darolutamide (Nubeqa) are androgenreceptor inhibitors that stop testosterone from binding to the cancer cells.
Studies published by the show these agents can add 1218 months of median survival when combined with standard hormone therapy.
Does chemotherapy help stage4 prostate cancer?
Yes especially for men with highvolume disease (many bone lesions) or rapidly rising PSA. The landmark CHAARTED trial proved that adding six cycles of docetaxel to hormone therapy can extend overall survival by roughly 23months, but for many, that extra time is packed with meaningful days.
Radiation Therapy (Targeted & Palliative)
Radiation isnt just for curative intent in early stages; it also plays a big role in stage4:
- Externalbeam radiation can shrink a painful bone metastasis, offering relief for weeks to months.
- Radium223 (Xofigo) is a radiopharmaceutical that homes in on bone lesions, delivering radiation directly to the tumor while sparing surrounding tissue.
Immunotherapy & Targeted Therapies
For a small slice of patients with specific genetic markers (e.g., MSIhigh or DNArepair defects), immunotherapy such as pembrolizumab or the vaccinetype sipuleucelT can be an option. Its not mainstream yet, but ongoing trials are promising.
Multimodal Combination Strategies
Many oncologists now favor a triplet approach: ADT (androgendeprivation therapy) + abiraterone + docetaxel. The ARASENS trial, released earlier this year, showed that this combo can push median survival beyond 5years for selected patients.
Sideeffect balance benefits vs. risks
Every treatment comes with tradeoffs:
- Hormone therapy can cause hot flashes, loss of libido, bone thinning, and mood changes.
- Docetaxel may lead to neutropenia (low white cells), nail changes, and fatigue.
- Radiation can cause skin irritation and occasional bowel issues if targeting pelvic nodes.
Proactive managementlike calcium & vitaminD supplements, regular bone density scans, and exercisehelps keep these sideeffects in check.
Personalizing Your Plan
Factors that shape the best treatment for you
Theres no onesizefitsall answer. Your doctor will weigh:
- The number and location of metastases.
- Overall health, heart and kidney function.
- Genetic findings a BRCA2 mutation, for instance, may point to PARP inhibitors as a supplemental option.
Questions to ask your oncology team
Feeling empowered starts with the right questions. Try asking:
- Will adding abiraterone improve my survival compared to hormone therapy alone?
- What impact will treatment have on my daily energy and mood?
- How often will we monitor PSA and imaging, and what will signal that we need to change tack?
Sample conversation script
Hey Dr.Smith, Ive read about combining hormone therapy with chemotherapy. Based on my bone scan showing three lesions, do you think a docetaxel regimen would give me a meaningful advantage, or should we start with newer hormonal agents first?
When to consider clinical trials
Clinical trials are the engine of progress. The currently lists several phaseIII studies testing nextgeneration androgenreceptor degraders and immunotherapy combos. If youre eligible, a trial could give you access to cuttingedge therapy that isnt yet widely available.
RealWorld Outcomes
Whats the longest someone has lived with stage4?
There are documented cases of men surviving 1012years after a stage4 diagnosis, especially when they responded well to early aggressive combination therapy and maintained a healthy lifestyle. These stories are outliers, but they remind us that the diseases trajectory can be longer than the median statistics suggest.
Patient anecdote: My dads journey
My dad started ADT in March 2021, added abiraterone in June, and after his PSA plateaued, he entered a clinical trial for a PARP inhibitor because of his BRCA2 mutation. Six months later, his pain subsided, his bone density stabilized with weekly zoledronic acid, and he reported feeling more like his old self. Hes now 73 and still active in his gardenproof that a welltailored plan can preserve both years and joy.
Lifestyle & supportive care that boost outcomes
Exercise, even moderate walking, can reduce fatigue and improve bone health. A Mediterraneanstyle diet rich in omega3 fatty acids, fruits, and vegetables is associated with slower disease progression. Psychological supportwhether through counseling, support groups, or mindfulness practiceshelps manage the emotional rollercoaster that accompanies a stage4 diagnosis. For patients considering life after definitive treatments, resources on survival without prostate can provide practical perspectives on recovery and longterm quality of life.
Trusted Sources
Credible medical references to cite
When you dive deeper, youll find reliable information on sites like the , the , and the . Their guidelines are updated regularly and reflect the latest evidence.
Expert quotes & interview ideas
Including insights from a medical oncologist (e.g., Dr.JohnSmith, MD, at MD Anderson) about how combination therapy has shifted the survival curve can add authority. A urologists perspective on when surgery may still play a role in oligometastatic disease gives a wellrounded view.
Transparency & disclosures
All data presented here are drawn from peerreviewed studies published up to 2024 and reputable cancer organization guidelines. When you discuss options with your doctor, ask them to point you to the original trial publications so you can see the evidence firsthand.
Conclusion
Finding the best treatment for prostate cancer stage4 isnt about a single magic drug; its about a thoughtfully assembled toolboxhormone therapy, newer androgentargeted agents, chemotherapy, radiation, and sometimes immunotherapytailored to your unique situation. Understanding the disease, weighing benefits against sideeffects, and staying engaged with your care team can give you the longest, highestquality life possible.
If youre navigating this journey, consider downloading a free Stage4 Prostate Cancer Treatment Planner (youll find it at the bottom of the page) to keep track of appointments, questions, and sideeffect management tips. And remember, youre not aloneshare your story, ask questions, and lets keep the conversation going. Your voice matters, and together we can turn uncertainty into informed hope.
FAQs
What is the first‑line treatment for stage 4 prostate cancer?
The backbone is androgen‑deprivation therapy (ADT). It’s usually started with LHRH agonists or antagonists, and most doctors add a next‑generation hormonal agent such as abiraterone, enzalutamide, apalutamide or darolutamide for stronger disease control.
When should chemotherapy be added to the regimen?
Docetaxel chemotherapy is recommended for men with high‑volume metastatic disease or rapidly rising PSA despite ADT. Clinical trials (CHAARTED, STAMPEDE) show a survival benefit of 2‑3 months, and many patients experience a meaningful slowdown of tumor growth.
Can radiation therapy help when the cancer has spread to the bones?
Yes. External‑beam radiation can relieve painful bone lesions, while radium‑223 (Xofigo) delivers targeted radiation to bone metastases and improves overall survival in patients with symptomatic bone‑only disease.
Are there any targeted or immunotherapy options for stage 4 prostate cancer?
For a small subset of patients with specific genetic alterations (e.g., MSI‑high, BRCA1/2, or other DNA‑repair defects), immunotherapy such as pembrolizumab or PARP inhibitors can be effective. Sipuleucel‑T is also approved for asymptomatic or minimally symptomatic metastatic disease.
What lifestyle changes can support treatment and improve quality of life?
Regular moderate exercise, a Mediterranean‑style diet rich in omega‑3s, adequate calcium/vitamin D intake, and quitting smoking all help maintain bone health, energy levels, and overall well‑being during treatment.