Hey there! If youve ever felt a nagging, stiffback pain that just wont quit, youre not alone. The good news? The ASAS (Assessment of SpondyloArthritis International Society) criteria give doctors a clear, evidencebased roadmap to decide whether that ache might actually be ankylosing spondylitis (now often called axial spondyloarthritis). In the next few minutes, well break down exactly what those criteria are, why they matter, and how they compare to older rules like the Modified New York criteria. Ready? Lets dive in no fluff, just the stuff you really need to know.
What Are ASAS Criteria
Definition & Purpose
The ASAS criteria are a set of classification rules designed for researchers and clinicians to identify patients with axial spondyloarthritis (axSpA) early in the disease course. Think of them as a welltested checklist that blends imaging findings with a handful of clinical clues. By applying the criteria, physicians can feel confident theyre catching the disease before irreversible damage sets in.
Two Classification Arms
ASAS works like a twotrack system:
- Imaging arm: Requires sacroiliac (SI) joint inflammation on MRI (or definite sacroiliitis on Xray) plus at least one clinical feature.
- Clinical arm: Requires at least two SpA (spondyloarthritis) features plus a positive HLAB27 test.
This dualapproach lets doctors diagnose patients even when MRI isnt available, as long as the clinical picture is strong enough.
Who Can Apply Them?
The criteria are aimed at adults under 45 years old who have had back pain for at least three months. Younger patients often present with subtle symptoms, so catching them early can be a gamechanger.
Quick Reference Table: Imaging vs. Clinical Arm
| Arm | Key Requirement | Additional Needed |
|---|---|---|
| Imaging | Active sacroiliitis on MRI OR definite sacroiliitis on Xray | 1 clinical SpA feature |
| Clinical | HLAB27 positive | 2 clinical SpA features |
Core Clinical Features
Inflammatory Back Pain
Picture this: morning stiffness that lasts longer than half an hour, improves once you start moving, and returns after periods of rest. Thats classic inflammatory back pain (IBP). Its one of the cornerstone features of the ASAS criteria.
Peripheral Manifestations
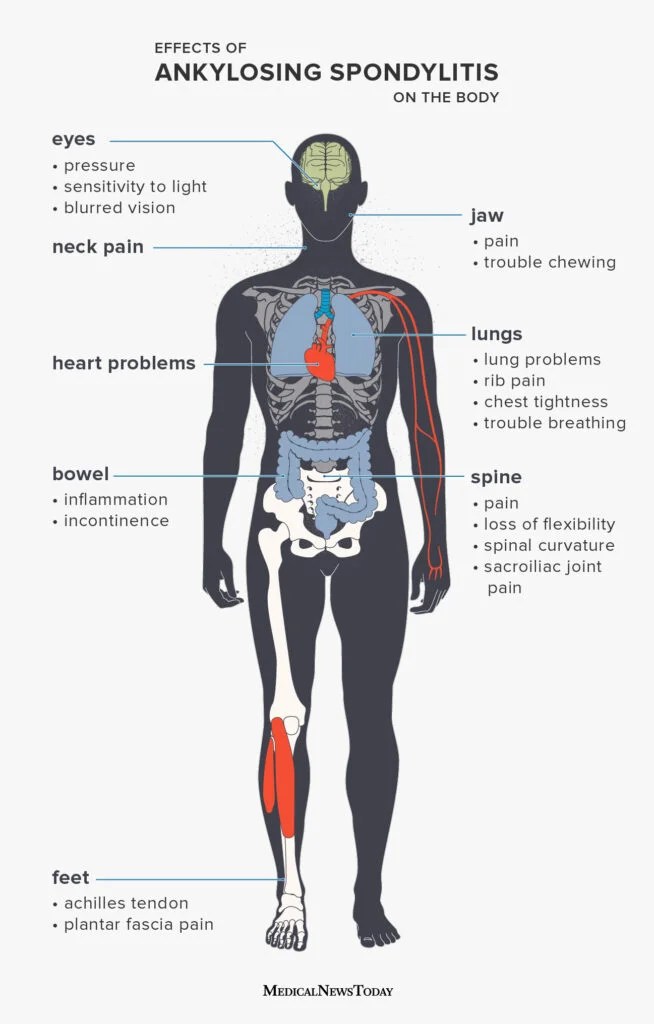
Even though ankylosing spondylitis primarily hits the spine, many patients also experience peripheral arthritis, enthesitis (tendontobone pain), or dactylitis (the sausage finger effect). Each of these counts toward the clinical arm.
ExtraArticular Signs
Things like acute anterior uveitis (eye inflammation), psoriasis, or inflammatory bowel disease (IBD) tip the scales. If youve ever heard a rheumatologist ask, Any eye problems lately? theyre hunting for these clues.
Family History & HLAB27
A positive HLAB27 test dramatically increases the odds that back pain is axSpA. However, a negative result doesnt rule it out about 1015% of patients are HLAB27 negative.
RealWorld Snapshot
Imagine a 32yearold office worker, Mike, who wakes up with a stiff lower back that eases after a coffeerun. He reports occasional heel pain and his sister has psoriasis. His MRI shows bonemarrow edema in the SI joints, and his lab work reveals HLAB27 positivity. Mike ticks the imaging arm (MRI + IBP) and the clinical arm (HLAB27 + peripheral sign), so he meets the ASAS criteria on both fronts.
Imaging Requirements Overview
MRI of the Sacroiliac Joints
MRI is the gold standard because it catches inflammation before structural damage appears on Xray. Radiologists look for bonemarrow edema, subchondral sclerosis, or erosions. The even offers a handy calculator to walk you through the imaging findings.
When Xray Suffices (Modified New York Criteria)
If the MRI isnt available, a plain radiograph can still be usefulbut only when it shows definite sacroiliitis (grade2 bilaterally or grade3 unilaterally). Those are the same thresholds used in the Modified New York criteria, which were the old benchmark before MRI entered the picture.
Spine MRI A Controversial AddOn
Some experts argue that adding spine MRI can improve sensitivity, especially when SI joint changes are subtle. However, studies (see the 2022 ASASEULAR recommendation) note that spine MRI alone often yields false positives, so its usually a secondary consideration.
Sample MRI Reporting Checklist
- Location of bonemarrow edema (right/left SI joint)
- Intensity and extent of signal change
- Presence of erosions, fatmetaplasia, or ankylosis
- Comparison with previous imaging, if any
Applying ASAS in Practice
StepbyStep Flow
1 Gather patient history focus on IBP, peripheral symptoms, extraarticular signs.
2 Order HLAB27 test.
3 If MRI is available, check for active sacroiliitis.
4 Use the table above to see which arm(s) the patient meets.
5 Document the classification and discuss treatment options.
Decision Tree for Ambiguous Cases
What if the MRI shows a tiny spot of edema that could be mechanical? In that scenario, look closely at the clinical arm if the patient has two or more SpA features plus HLAB27 positivity, you can still classify them as axSpA. Conversely, a positive MRI with no clinical features might warrant a watchandwait approach and repeat imaging in 612months.
Practical Example with Numbers
Patient Sara has:
- IBP (yes)
- Enthesitis at the Achilles (yes)
- HLAB27 negative
- MRI shows bonemarrow edema in the left SI joint
She meets the imaging arm (MRI + IBP). Even without HLAB27, she qualifies for the ASAS criteria and can be started on a biologic if symptoms are severe. If Sara and her clinician are discussing longterm goals like reducing symptoms and aiming for ankylosing spondylitis remission, they can track response using standardized remission measures and followup imaging when appropriate.
ASAS vs New York
Sensitivity & Specificity Snapshot
Research shows the ASAS criteria have a sensitivity of roughly 85% and a specificity of about 90% for early disease, while the Modified New York criteria lag behind with sensitivity near 70% (especially in the first two years of symptoms). The higher sensitivity means you catch more patients early, but you also need to be vigilant about false positives.
Advantages of ASAS
- Detects disease before radiographic changes appear.
- Incorporates MRI a modern imaging modality.
- Allows classification without imaging if the clinical picture is strong.
When New York Still Helps
If youre in a resourcelimited clinic where MRI isnt feasible, the Modified New York criteria can still serve as a fallback. Theyre also sometimes required for insurance coding in certain countries.
SidebySide Comparison Table
| Feature | ASAS Criteria | Modified New York |
|---|---|---|
| Age limit | 45y | Any age |
| Imaging needed | SIjoint MRI or Xray | Definite sacroiliitis on Xray |
| Clinical requirement | 1 SpA feature (Imaging arm) or 2 SpA features + HLAB27 (Clinical arm) | 2 clinical features (low back pain, limited motion) + Xray |
| Sensitivity (early disease) | 85% | 70% |
Benefits and Risks
Benefits
Using the ASAS criteria helps you diagnose axSpA sooner, which means patients can start diseasemodifying therapies (like TNF inhibitors) before irreversible spinal fusion occurs. Early treatment also improves quality of life, functional ability, and work productivity.
Risks / Limitations
The biggest caution is overdiagnosis. Some people have MRI changes that mimic inflammation but are actually mechanical or related to pregnancy. Relying solely on imaging without a solid clinical backdrop can lead to unnecessary medication exposure.
Mitigation Strategies
- Always verify that MRI findings match the clinical picture.
- Repeat imaging if the first scan is equivocal.
- Consider alternative diagnoses (e.g., mechanical lowback pain, osteitis condensans ilii).
- Use a shared decisionmaking approach with the patient.
Key Helpful Resources
Online Calculators & Apps
The lets you input symptoms and imaging results to see instantly whether the criteria are met.
Authoritative PDFs & Guidelines
The official ASAS Handbook (available from the ASAS website) and the 2022 ASASEULAR management recommendations provide the most uptodate evidencebased guidance.
PatientFriendly Handouts
Many rheumatology societies offer printable fact sheets that explain axSpA in plain language. These can be great for bringing a friend or family member into the conversation.
QuickDownload CheatSheet
Weve prepared a onepage PDF that summarizes the imaging arm, the clinical arm, and the key redflag symptoms. Download it, stick it on your fridge, and youll never forget what to look for.
Conclusion
In a nutshell, the ASAS criteria give clinicians a reliable, earlystage roadmap to identify ankylosing spondylitis (axial spondyloarthritis). By blending MRI or Xray findings with a handful of clinical clues inflammatory back pain, peripheral signs, extraarticular features, and HLAB27 status the criteria outperform the older Modified New York system, especially in younger patients. Yet, as with any diagnostic tool, balance is key: use the criteria as a guide, not a verdict, and always consider the whole patient story.
Ready to put this knowledge into practice? Grab the cheatsheet, run a quick check with the MDCalc calculator, and discuss the results with your rheumatology team. Early detection can change the trajectory of the disease and thats something worth celebrating.
FAQs
What is the purpose of the ASAS criteria?
The ASAS criteria provide a standardized way to identify axial spondyloarthritis early, using MRI findings, clinical features, and HLA‑B27 status.
Who can be classified using the ASAS criteria?
Adults 45 years or younger with chronic back pain lasting ≥ 3 months are eligible; the criteria aim to catch disease in its early phase.
What are the two arms of the ASAS classification?
One arm requires active sacroiliitis on MRI (or definitive sacroiliitis on X‑ray) plus ≥ 1 clinical feature; the other needs HLA‑B27 positivity plus ≥ 2 clinical features.
How does MRI improve early detection compared to the Modified New York criteria?
MRI can show inflammatory changes before structural damage appears on X‑ray, increasing sensitivity to about 85 % versus ~70 % for the older criteria.
Can a patient be classified without an MRI?
Yes—if they are HLA‑B27 positive and have at least two other SpA features, they meet the clinical arm of the ASAS criteria.