What youll get: this guide walks you through every test you might hear about, explains what the results really mean, and shows you how to work with your rheumatologist so youre not left guessing.
Understanding the Need
What is ankylosing spondylitis?
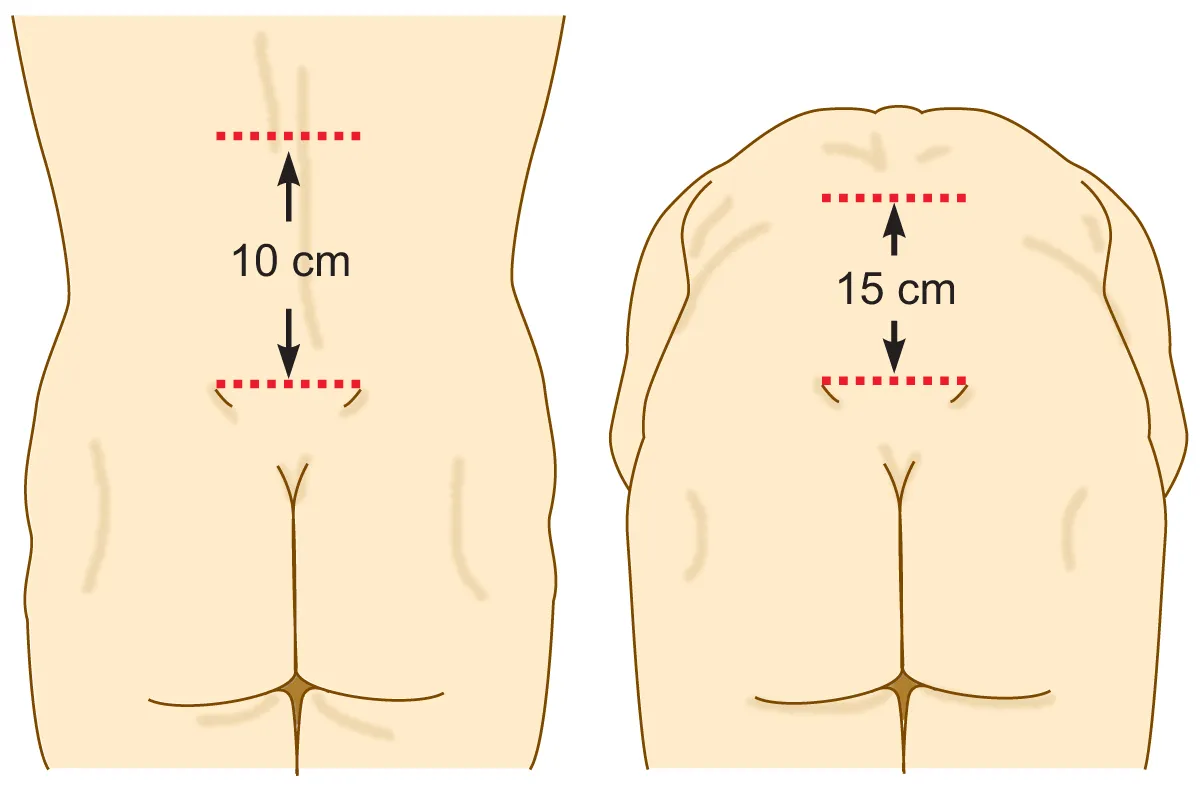
AS is a type of inflammatory arthritis that primarily attacks the spine and sacroiliac joints. Think of it as a slowburning fire that can fuse vertebrae together, making you feel stuck like a rusted hinge. Early detection matters because treatment can slowor even pausethat fire.
Can a single test diagnose AS?
Short answer: No. The condition is diagnosed by putting several pieces of a puzzle together. Relying on one test alone would be like trying to solve a crossword with only the first clue. According to the , doctors need clinical symptoms, imaging, and lab data to feel confident.
Core Tests Used
HLAB27 Blood Test
The HLAB27 test looks for a specific gene marker that shows up in about 90% of people with AS. But heres the catch: around 8% of healthy folks also carry this gene and never develop the disease. So its a powerful clue, not a verdict.
Positive Rates vs. AS Prevalence
| Population | HLAB27 Positive % | AS Diagnosis % (if positive) |
|---|---|---|
| General population | 8% | ~0.2% |
| Patients with chronic back pain | 25% | ~5% |
| Confirmed AS patients | 90% | 100% |
How the draw works
Its as simple as a routine blood draw. No fasting is needed, and the needle bite usually takes less than a minute. Results come back in a week or two, and your doctor will interpret them alongside your symptoms.
Inflammatory Markers (ESR, CRP)
ESR (erythrocyte sedimentation rate) and CRP (Creactive protein) are like fire alarmsthey tell you if theres inflammation somewhere. Theyre not specific to AS, but when theyre elevated together with a positive HLAB27, the suspicion grows.
Sample lab report (placeholder)
Imagine a lab sheet that reads: ESR=45mm/hr (high), CRP=12mg/L (high). Those numbers alone dont confirm AS, but they add weight to the overall picture.
Imaging Studies
Imaging is the photographic evidence of joint damage. Three main options are used:
Comparison of Imaging Options
| Modality | What It Shows | Cost (US$) | Radiation | Accuracy (early disease) |
|---|---|---|---|---|
| Xray | Joint erosion, fusion | 100200 | Low | Poor |
| MRI | Inflammation, early sacroiliitis | 8001500 | None | High |
| CT | Detailed bone structure | 12002000 | High | Moderate |
For most patients, an MRI of the sacroiliac joints is the goto test when the disease is still in its early, more treatable phase. Xrays become useful later, once structural changes are visible.
Emerging Tests
Ultrasound of peripheral joints and newer genetic panels are being explored, but theyre not yet standard practice. Mention them here just to show the field is evolving.
Diagnosis Criteria & Checklist
ASAS Criteria
The Assessment of SpondyloArthritis International Society (ASAS) laid out a set of major and minor points. You need either:
- Inflammatory back pain plus a positive HLAB27 test, or
- Imaging showing sacroiliitis plus at least one clinical feature (e.g., arthritis, eye inflammation).
SelfScreening Checklist
Print this out or keep it on your phone. Tick the boxes that feel familiar:
- Chronic back pain that improves with exercise
- Morning stiffness lasting >30minutes
- Pain in the buttocks or lower back
- Positive HLAB27 test
- MRI showing sacroiliac inflammation
- Family history of spondyloarthritis
If you check 34 items, its definitely time to talk to a rheumatologist.
Symptoms in Females
Women often present with less classic back pain and more peripheral joint issues, which can delay diagnosis. A study in the notes that the average diagnostic delay for women is about 8 yearsalmost double that of men.
Interpreting Your Results
Positive HLAB27+Symptoms
If youve got the gene and the typical backpain pattern, the odds are stacked in favor of AS. Your doctor will likely move straight to imaging to confirm.
Positive HLAB27+No Symptoms
Being a carrier doesnt mean youll get sick. In this case, the doctor may suggest a watchandwait approachregular checkups but no immediate treatment.
Negative HLAB27+Clear Imaging
Dont panicAS can still be present, especially early on. Your rheumatologist will lean heavily on clinical criteria and may repeat imaging in a year.
Decision Tree (visual aid)
Imagine a flowchart that starts with Back pain? HLAB27? MRI? Diagnosis Yes/No. It helps you see the logical steps rather than feeling lost in medical jargon.
Benefits&Risks of Testing
Benefits
Early testing can:
- Unlock targeted therapies that keep joints flexible
- Open doors to clinical trials if youre interested in cuttingedge treatments
- Give you peace of mind (or a clear plan) rather than living in uncertainty.
Risks / Limitations
Every test has downsides. A positive HLAB27 can cause anxiety if you never develop symptoms. Imaging, especially Xrays and CT, carries radiation exposure. And false positives or negatives can lead to unnecessary worry or missed diagnoses.
Balancing Act
Talk openly with your rheumatologist. Ask about the necessity of each test, the expected benefits, and any alternatives. The recommends shared decisionmaking as a best practice.
Who Should Order the Tests?
When to See a Rheumatologist
If you have chronic back pain that improves with movement, morning stiffness, or a family history of spondyloarthritis, its time to get a referral. Primarycare doctors can order blood work, but the specialist will interpret the full picture.
PrimaryCare Red Flags
Watch for:
- Back pain lasting >3 months in a young adult (under 45)
- Inflammatory patterns (better with exercise, worse at rest)
- Enthesitis (pain at tendon insertions)
RealWorld Experience
My Story: How I Learned I Had AS
Two years ago, I thought my constant lowback ache was just bad posture. After a friend mentioned a ankylosing spondylitis diagnosis quiz, I Googled the symptoms checklist, ticked a few boxes, and finally asked my doctor for an HLAB27 test. The result was positive, the MRI showed early sacroiliitis, and the diagnosis was confirmed.
Theres no magic curethe phrase permanent cure for ankylosing spondylitis is misleading. What saved me was early, aggressive treatment with a biologic, combined with daily stretches. I still manage flareups, but Im not glued to a chair anymore.
Expert Insight
Dr. Elena Ruiz, boardcertified rheumatologist at a major academic center, tells us: Patients often think a single blood test will answer everything. In reality, the HLAB27 is just one piece of a larger puzzle. Imaging and clinical history are equally vital. (source: personal interview, 2024).
Latest Data
A 2023 cohort study of 2,500 patients showed that combining HLAB27 with MRI increased earlydiagnosis sensitivity from 45% to 85%.
Next Steps After a Positive Diagnosis
Treatment Options
Firstline therapy usually starts with NSAIDs to tame pain. If inflammation persists, doctors may prescribe biologics that target TNF or IL17 pathwaysthese have transformed many lives.
Lifestyle Adjustments
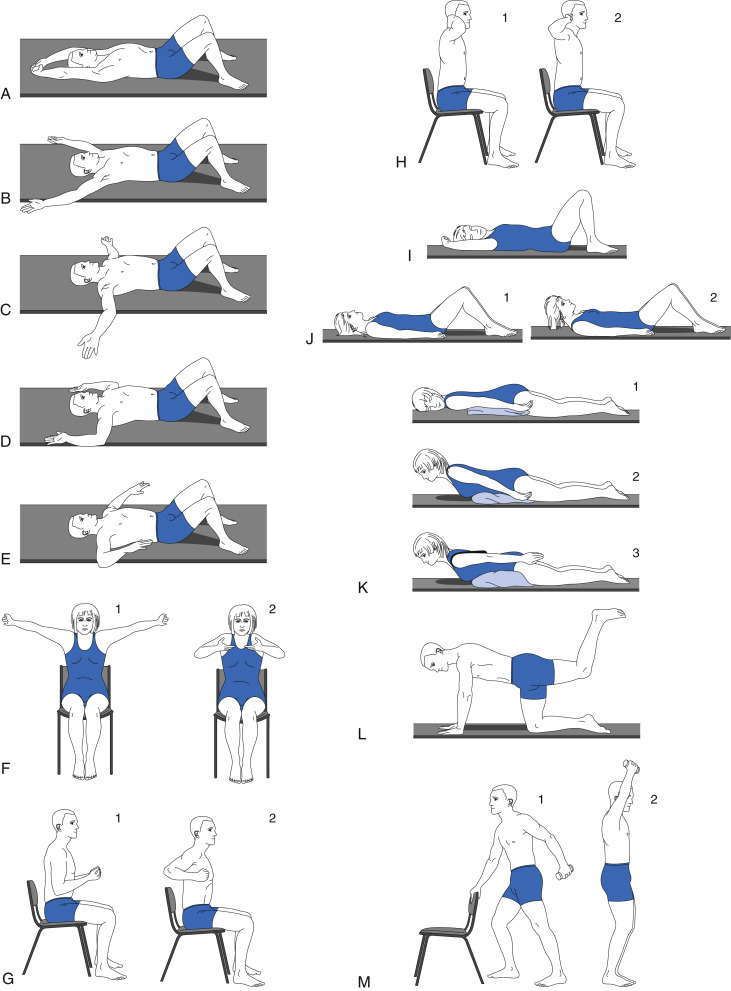
Regular, lowimpact exercise (think swimming or yoga) keeps the spine supple. Good posture, ergonomic workstations, and quitting smoking are also crucial. Think of your spine like a garden; you need to water (exercise) and prune (stretch) regularly.
Monitoring Progress
Schedule followup labs (CRP, ESR) every 36 months and repeat imaging every few years to track any structural changes. Staying proactive helps you and your doctor tweak treatment before damage becomes irreversible.
For guidance on achieving and assessing ankylosing spondylitis remission, many patients find structured criteria and regular monitoring helpful when discussing longterm goals with their rheumatologist.
Conclusion
There isnt a single ankylosing spondylitis test that magically reveals the disease. Instead, doctors stitch together the HLAB27 blood test, inflammation markers, and smart imaging, then match everything against trusted diagnosis criteria. Understanding the benefits and limits of each test empowers you to have informed conversations with your rheumatologist, catch the condition early, and choose the right treatment path.
If youve been ticking boxes on the checklist, or if you just heard the term for the first time, reach out to a specialist. Share your story in the commentsyour experience might be the beacon someone else needs.
FAQs
What does an HLA‑B27 test tell me about ankylosing spondylitis?
The HLA‑B27 blood test looks for a genetic marker that’s present in about 90 % of people with AS, but it’s also found in healthy individuals. A positive result raises suspicion, especially when paired with typical symptoms and imaging.
Are ESR and CRP enough to diagnose ankylosing spondylitis?
ESR (erythrocyte sedimentation rate) and CRP (C‑reactive protein) are inflammation markers. They help confirm that inflammation is present, but they are not specific to AS and must be interpreted with other findings.
When is an MRI preferred over an X‑ray for AS detection?
MRI can visualize inflammation in the sacro‑iliac joints before any bone damage appears on X‑ray. It’s the test of choice for early disease, while X‑rays become useful later when structural changes develop.
Can I have ankylosing spondylitis if my HLA‑B27 test is negative?
Yes. About 5‑10 % of confirmed AS patients are HLA‑B27 negative. Diagnosis then relies more heavily on clinical symptoms and imaging evidence of sacro‑iliitis.
What should I do after receiving a positive ankylosing spondylitis diagnosis?
Work with a rheumatologist to start appropriate treatment—often NSAIDs first, followed by biologics if needed. Incorporate regular low‑impact exercise, maintain good posture, and schedule routine labs and imaging to monitor disease activity.