Understanding the Illness
What causes acute gastroenteritis?
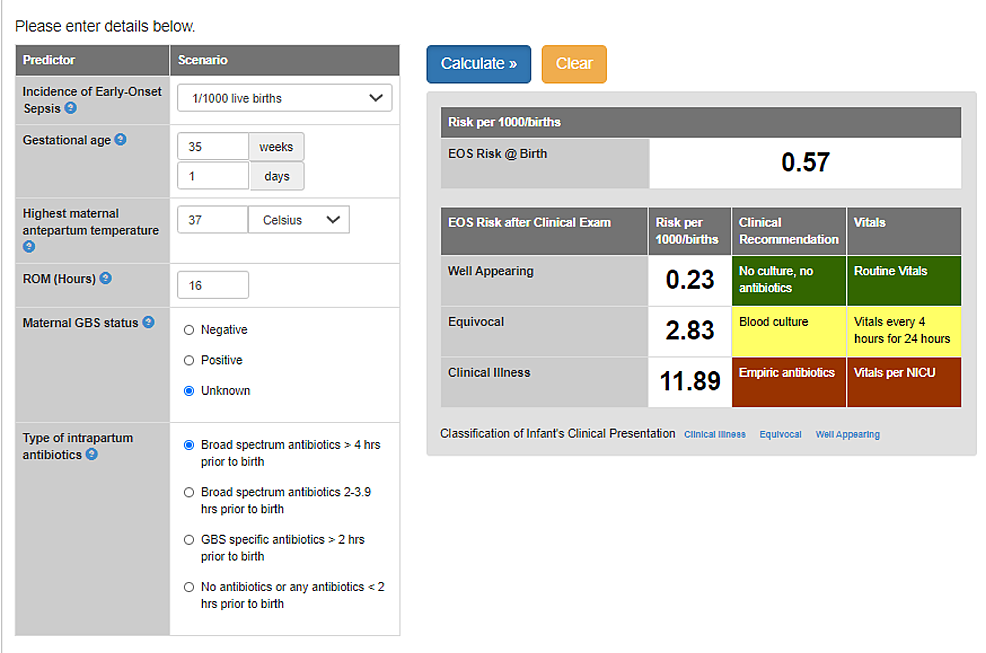
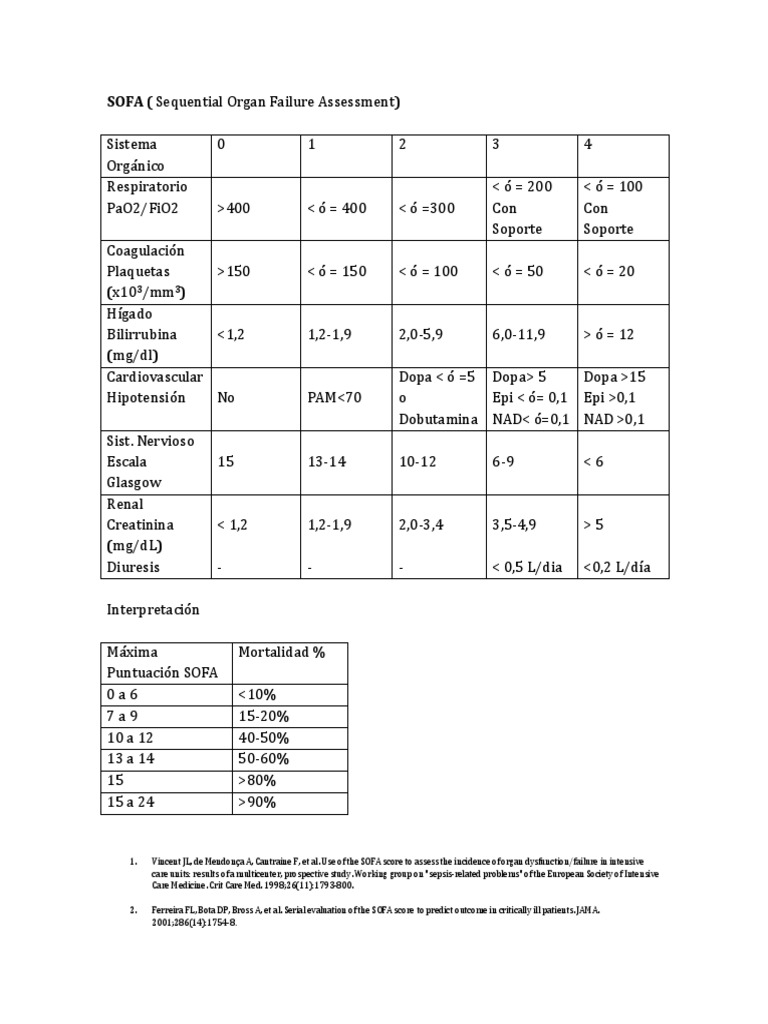
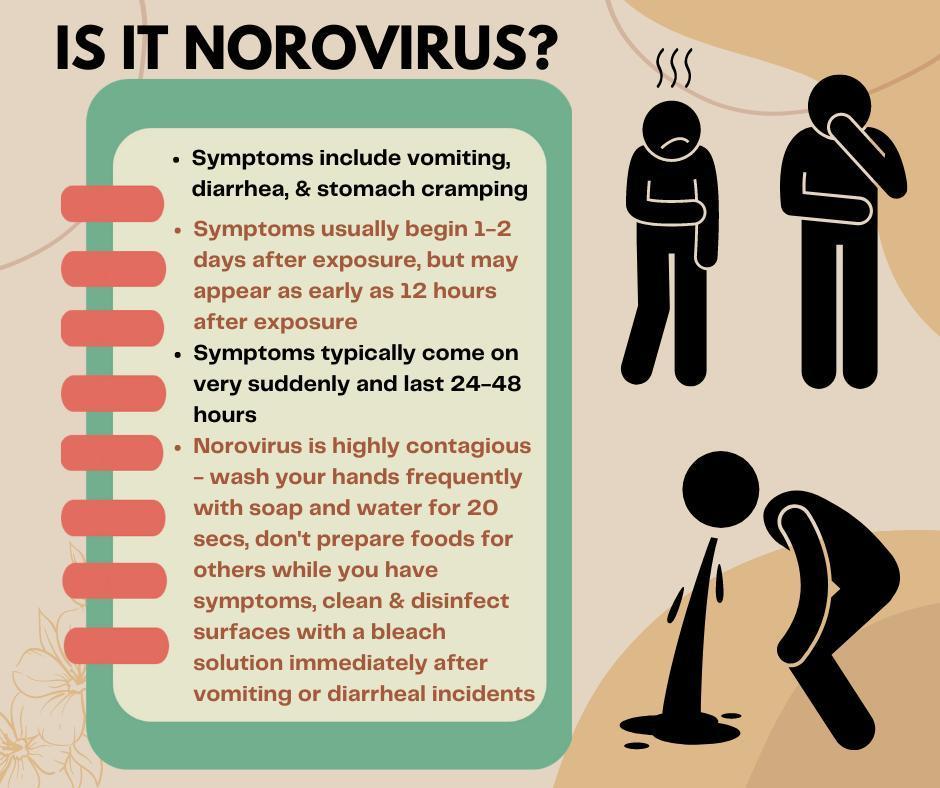
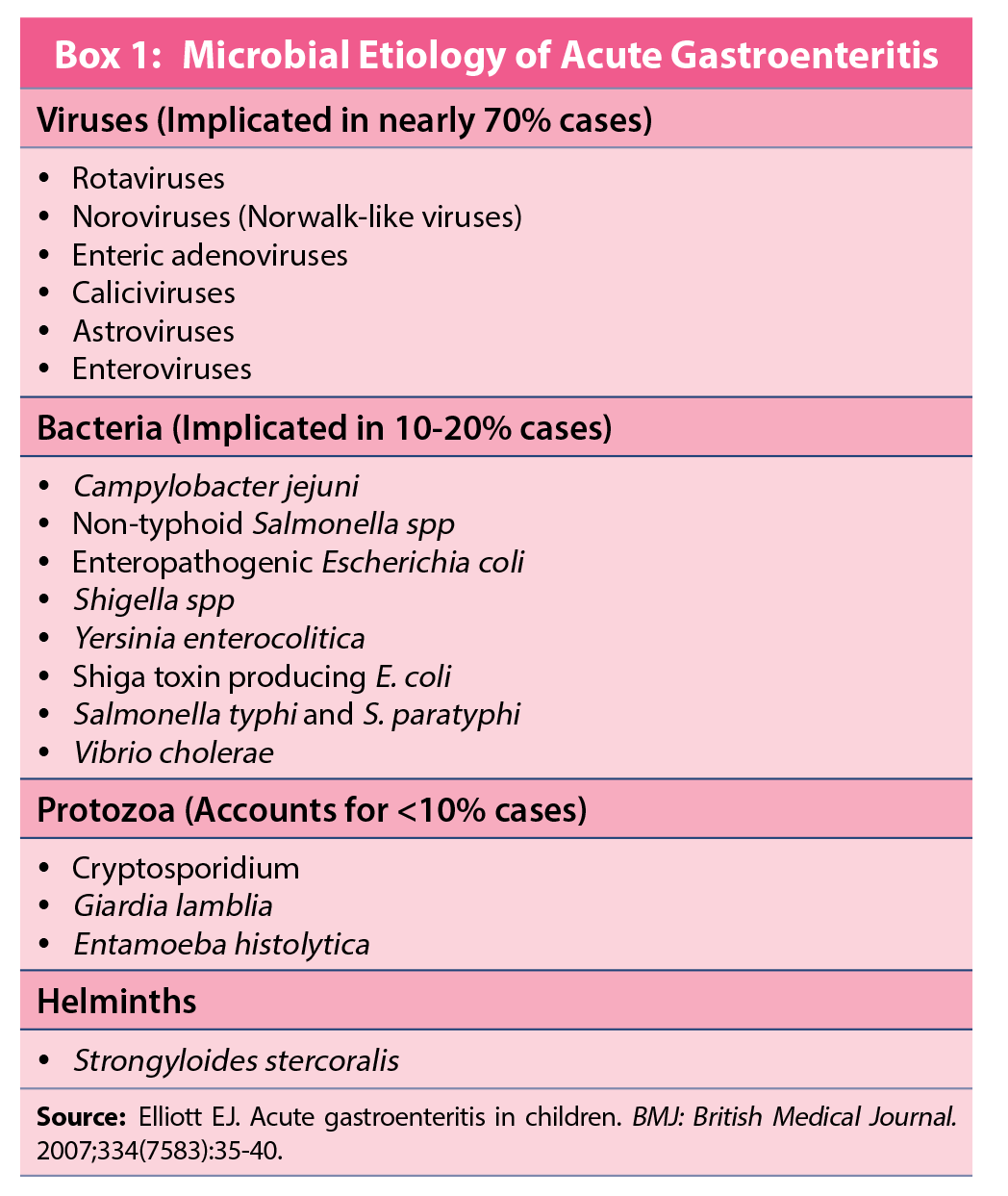
Acute gastroenteritis is an inflammation of the stomach and intestines that usually shows up as diarrhea, vomiting, and cramps. The culprit is often a virusthink norovirus or rotavirusbut bacteria (like Campylobacter, Salmonella, or Shigella) and even parasites can be responsible. According to the , viruses account for roughly 70% of cases in the United States, while bacterial causes make up about 20%. For guidance on when symptoms suggest a more severe infection, clinicians sometimes use tools from sepsis and organ failure assessment frameworks such as the organ failure assessment to evaluate systemic involvement.
Typical symptoms and redflag signs
- Watery diarrhea lasting<3days (usually viral)
- Fever>38.5C, especially with bacterial infection
- Blood or mucus in stool a clear warning sign
- Severe abdominal pain or persistent vomiting
- Dehydration (dry mouth, dizziness, reduced urine output)
Realworld glimpse
Imagine Mark, a 28yearold who returned from a hiking trip in the Pacific Northwest. He developed highgrade fever, bloody diarrhea, and severe cramping. A stool culture revealed Campylobacter jejuni. In Marks case, antibiotics were a lifesaver, whereas most of his fellow travelers recovered without them.
Antibiotics Role
Why antibiotics arent routine
Most acute gastroenteritis cases are viral, and antibiotics simply dont work against viruses. A 2023 guideline from the stresses that unnecessary antibiotic use can lead to resistance, gutflora disruption, and even Clostridioides difficile infection. In short, taking a pill when you dont need it is like using a sledgehammer to crack a walnutwasteful and risky.
Evidence snapshot
Most mild infections will recover without antibiotics. Moderatetosevere cases should be treated with targeted therapy, notes a Medscape review on bacterial gastroenteritis antibiotics. This balance between benefit and harm is the core of the gastroenteritis antibiotics guidelines that clinicians follow.
Risks of unnecessary treatment
Beyond antibiotic resistancea global health nightmarethere are more immediate concerns:
- Allergic reactions (from mild rash to anaphylaxis)
- Sideeffects like nausea, abdominal pain, and dizziness
- Disruption of the good bacteria that keep our gut happy
- Potential overgrowth of C.difficile, causing severe colitis
Quick visual aid (imagine)
If you were to draw a sidebyside chart, youd see faster symptom resolution with antibiotics in confirmed bacterial cases, but also a higher rate of sideeffects in viral cases where the drug was unnecessary.
When to Treat
Spotting bacterial gastroenteritis
The key is a combination of clinical clues and lab tests. Blood or mucus in stool, high fever, and a recent travel history raise suspicion. Confirmatory stool culture, PCR panels, or rapid antigen tests can pinpoint the pathogen.
Clinical scenarios that merit antibiotics
- Severe dehydration that doesnt improve with oral rehydration
- Immunocompromised patients (e.g., chemotherapy, HIV)
- Dysentery caused by Shigella or enteroinvasive E.coli
- Travelrelated infections like cholera or severe Campylobacter
- Persistent symptoms >7days with confirmed bacterial cause
Decisiontree (quick mental model)
1Assess hydration 2Check for blood/mucus 3Order stool test if redflags 4If bacterial confirmed, select appropriate antibiotic 5Monitor response.
Adult Options
Firstline: ampicillin
When the pathogen is susceptible, ampicillin (500mg every 6hours for 35days) remains a solid choice. Its inexpensive and widely available, but resistance patterns vary by region.
TableA Ampicillin vs. resistance (2024 CDC data)
| Pathogen | Resistance Rate | Comment |
|---|---|---|
| Salmonella spp. | 12% | Generally effective |
| Shigella flexneri | 27% | Consider alternatives if >20% |
| Campylobacter jejuni | 35% | Often resistant azithromycin preferred |
Alternatives for resistant strains or penicillin allergy
- Trimethoprimsulfamethoxazole (TMPSMX) ideal for many resistant bacteria; dose 160/800mg BID for 3days.
- Azithromycin 500mg once daily for 3days; especially useful for travelrelated Campylobacter.
- Ciprofloxacin 500mg BID, but rising fluoroquinolone resistance limits its use.
Comparison chart best antibiotic for gastroenteritis?
| Drug | Efficacy | Sideeffects | Cost |
|---|---|---|---|
| Ampicillin | High (susceptible strains) | GI upset, rash | Low |
| TMPSMX | Moderatehigh | Allergic rash, rare blood issues | Lowmoderate |
| Azithromycin | High for travel bugs | Mild GI, rare QT prolongation | Moderate |
| Ciprofloxacin | Variable | Tendinitis, tendon rupture | Low |
Expert insight
Dr. Laura Chen, an infectiousdisease specialist, notes, When choosing between TMPSMX and azithromycin, I look at the patients travel history and any known drug allergies. Azithromycins oncedaily dosing often improves adherence.
Child Options
Best antibiotic for a childs stomach infection
For children, amoxicillin is the goto when the isolate is susceptible. A typical pediatric dose is 25mg/kg per dose every 8hours for 5days. Its welltolerated and has a long safety record.
Pediatric dosing table
| Age | Weight (kg) | Amoxicillin dose (mg/kg/day) | Frequency |
|---|---|---|---|
| 6months 2years | 1012 | 25 | Every 8h |
| 25years | 1218 | 25 | Every 8h |
| 612years | 2040 | 25 | Every 8h |
When to switch from amoxicillin
If a child has a documented penicillin allergy, options include cotrimoxazole (TMPSMX) or azithromycin. The dose for azithromycin is 10mg/kg on day1, then 5mg/kg on days24.
Story from the clinic
Little Maya, 4years old, presented with dysentery and a known amoxicillin allergy. After a rapid stool PCR identified Shigella, her pediatrician prescribed azithromycin. Within 48hours, her fever fell and stools clearedproof that the right drug matters, even for the tiniest patients.
Guidelines Overview
Adult treatment guidelines (AAFP 2024)
The American Academy of Family Physicians advises:
- Start with aggressive oral rehydration.
- Reevaluate after 48hoursif symptoms persist and bacterial infection is confirmed, initiate antibiotics.
- Choose firstline agents based on local resistance patterns; switch if no improvement.
Child treatment guidelines (AAP 2023)
Key points for children:
- Prioritize oral rehydration solutions (ORS) before any medication.
- Reserve antibiotics for confirmed bacterial infection or severe dehydration.
- Use amoxicillin as first choice; adjust for allergy or resistance.
Downloadable checklist (imagine a PDF)
Think of a handy, printable checklist that walks you through hydration, redflag assessment, testing, and antibiotic decisionmaking. Its the kind of tool doctors love to hand out after an office visit.
Side Effects & Monitoring
Common adverse effects
Even the friendliest antibiotics can cause:
- Stomach upset and diarrhea (paradoxical, right?)
- Skin rash or mild itching
- Rarely, photosensitivity or liver enzyme elevations
Tips to minimize trouble
Take antibiotics with food (unless the label says otherwise), stay hydrated, and consider a probiotic supplement to keep the good bacteria in check. Some clinicians recommend a short course of Lactobacillus during and after treatment.
When to stop early
If you experience any of the following, call your healthcare provider immediately:
- Severe rash or swelling of the face/lips
- Difficulty breathing
- Persistent vomiting that prevents medication absorption
- New onset of severe abdominal pain
Physicians note
A 48hour reassessment is crucial, advises Dr. Ahmed Patel, a gastroenterologist. If theres no clinical improvement, we either change the antibiotic based on culture results or consider that the infection might be viral, prompting us to stop the drug.
Key Takeaways
Heres the distilled wisdom you can walk away with:
- Most acute gastroenteritis cases dont need antibioticshydration and rest are often enough.
- Reserve acute gastroenteritis antibiotics for confirmed bacterial infections, severe dehydration, or highrisk patients.
- For adults, ampicillin is firstline when susceptible; azithromycin shines for travelrelated bugs, while TMPSMX covers many resistant strains.
- Children typically receive amoxicillin; if allergic, azithromycin or cotrimoxazole are solid alternatives.
- Always follow evidencebased guidelines (AAFP, AAP) and let a clinician interpret lab results before starting therapy.
Remember, antibiotics are powerful toolsbut like any tool, they work best when used wisely. If youre ever in doubt, reach out to your doctor, share your symptoms, and let the labs guide the treatment. Your gutand the communitys antimicrobial futurewill thank you.
Whats your experience with gastroenteritis? Have you ever been prescribed an antibiotic that turned out unnecessary, or did the right drug make a quick recovery? Share your story in the comments below; wed love to hear from you!
FAQs
How can I tell if my gastroenteritis needs antibiotics?
Look for red‑flag signs such as high fever, blood or mucus in stool, severe abdominal pain, persistent vomiting, or confirmed bacterial infection from a stool culture or PCR test. In the absence of these, supportive care is usually sufficient.
What are the first‑line antibiotics for adults with bacterial gastroenteritis?
Ampicillin (500 mg q6h for 3–5 days) is often the initial choice when the pathogen is susceptible. If resistance is common or the patient is allergic to penicillins, azithromycin or trimethoprim‑sulfamethoxazole are common alternatives.
Which antibiotic is safest for children with acute gastroenteritis?
Amoxicillin (25 mg/kg/dose every 8 hours for 5 days) is the preferred agent for susceptible bacteria. For children with a penicillin allergy, azithromycin (10 mg/kg day 1 then 5 mg/kg days 2‑4) or TMP‑SMX can be used.
How long should I take antibiotics for a confirmed bacterial infection?
Typical courses range from 3 to 5 days for most bacterial pathogens. Some infections (e.g., severe Campylobacter) may require up to 7 days. Always follow the prescribing clinician’s instructions and complete the full course.
Can taking antibiotics for gastroenteritis cause other problems?
Yes. Unnecessary use can lead to antibiotic resistance, disrupt normal gut flora, cause side‑effects like rash or nausea, and increase the risk of Clostridioides difficile infection. Use them only when clearly indicated.