Active psoriatic arthritis (active PsA) means the joint inflammation tied to psoriasis is currently flaring causing pain, swelling, or stiffness that disrupts your daytoday life. Spotting the early warning signs, understanding the five disease patterns, and getting the right treatment can keep those flares in check and protect your joints for the long haul.
What Is Active
When doctors talk about active PsA, theyre describing a state where the inflammation isnt dormant. In other words, the disease is doing its job of irritating joints, tendons, and even the skin. This differs from remission, where symptoms are minimal or gone altogether. For patients aiming for sustained improvement, understanding AS remission criteria can help set treatment goals and guide decisions about stepping down therapy.
How Doctors Measure Activity
Rheumatologists use a few standard tools:
- DAS28 (Disease Activity Score) looks at 28 joints for tenderness and swelling.
- PASI (Psoriasis Area Severity Index) evaluates skin involvement.
- Patientreported outcome measures simple questionnaires that ask how you feel on a daytoday basis.
Activity Level Table
| Level | DAS28 Score | PASI Score | Typical Symptoms |
|---|---|---|---|
| Low | 2.6 | 3 | Occasional joint ache, mild skin patches |
| Moderate | 2.73.2 | 47 | Frequent swelling, noticeable stiffness |
| High | >3.2 | >7 | Severe pain, joint damage risk, extensive skin lesions |
Understanding where you land on this scale helps you and your doctor decide how aggressively to treat the disease.
Early Warning Signs
Knowing the early signs can feel like having a radar for a storm thats just forming. Catch it early, and you can steer clear of the worst of it.
Six Core Early Signs
- Pain or tenderness in joints, especially after rest.
- Swelling that doesnt disappear with rest.
- Morning stiffness lasting more than 30 minutes.
- Changes in nail appearance pitting, thickening, or separation.
- Red, scaly skin patches (psoriasis) that may appear before joint pain.
- Enthesitis pain where tendons attach to bone, often at the heel or elbows.
Early Signs in the Feet
The feet are a sneaky spot. Many people first notice a painful heelburn or swelling along the outer edge of the foot, which can be mistaken for a simple sprain. If your feet feel like theyre on fire after a day of standing, you might be experiencing the early signs of psoriatic arthritis in the feet.
A Quick Story
Imagine Sarah, a graphic designer who loved marathon running. She chalked up a lingering heel pain to overtraining, but the ache grew into swelling and difficulty walking. After months of itll go away, a rheumatologist diagnosed her with active PsA. Catching it early saved her from irreversible joint damage and allowed her to modify training rather than quit running altogether.
How to Differentiate From Other Conditions
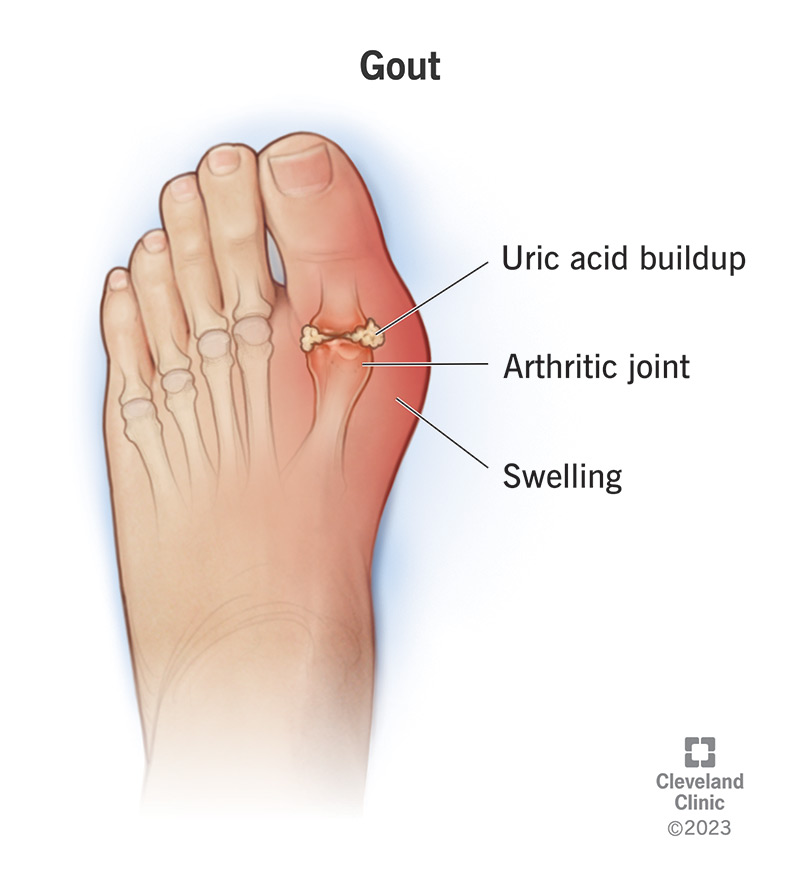
Joint pain can stem from osteoarthritis, gout, or even a simple injury. Heres a handy checklist:
- Pattern PsA often affects the distal joints (fingers, toes) and may be asymmetric.
- Nail changes Rare in osteoarthritis, common in PsA.
- Skin involvement Psoriasis plaques are a big giveaway.
- Enthesitis Tenderness at tendon insertions is a PsA hallmark.
Five Types Explained
Psoriatic arthritis isnt onesizefitsall. In fact, there are five recognized patterns, each with its own personality. Knowing which one you have can shape treatment decisions.
Overview of the Five Patterns
- Dactylitis (Sausage Digits) Swelling of an entire finger or toe.
- Axial Involvement Inflammation of the spine and sacroiliac joints.
- Asymmetric Oligoarthritis A few joints on one side of the body.
- Symmetric Polyarthritis Many joints on both sides, mimicking rheumatoid arthritis.
- Arthropathic Psoriasis Skin disease dominates, with occasional joint flareups.
Comparison Table
| Type | Typical Joints | Common Onset Age | Imaging Clues |
|---|---|---|---|
| Dactylitis | Digits (fingers/toes) | 2040 | Uniform swelling on Xray |
| Axial | Spine, sacroiliac | 3050 | Bone erosion on MRI |
| Asymmetric Oligo | Few peripheral joints | 1535 | Localized inflammation |
| Symmetric Poly | Many peripheral joints | 4060 | Joint space narrowing similar to RA |
| Arthropathic | Skin predominates | Any | Minimal joint changes early |
Which Type Is Most Often Active?
Axial involvement and dactylitis tend to produce the most noticeable active disease because they affect large, functional areas (the spine and hands). If youre dealing with persistent back pain or a sausagelike finger, chances are your PsA is in an active phase.
Diagnosis Process
Getting a clear diagnosis is a bit like detective work you need clues from the history, a keen eye on imaging, and some lab tests to rule out impostors.
Clinical Evaluation
Your doctor will start with a detailed conversation about skin lesions, joint pain patterns, and family history. The physical exam often includes checking nail changes and looking for enthesitis at common sites.
Imaging Studies
- Xrays Good for spotting bone erosion in later stages.
- Ultrasound Detects early softtissue swelling and synovitis.
- MRI The gold standard for axial disease and hidden inflammation.
Blood & Lab Tests
Unlike rheumatoid arthritis, PsA is usually , meaning rheumatoid factor tests come back negative. Doctors often check Creactive protein (CRP) and erythrocyte sedimentation rate (ESR) to gauge inflammation, and may look for the HLAB27 gene if axial involvement is suspected.
Diagnostic Flowchart
| Step | Action | Purpose |
|---|---|---|
| 1 | Medical history & physical exam | Identify pattern, nail/skin clues |
| 2 | Blood tests (CRP, ESR, RF) | Rule out other arthritis types |
| 3 | Imaging (Xray, US, MRI) | Visualize joint damage & inflammation |
| 4 | Diagnosis confirmation | Set treatment plan |
Treatment Options
Theres no onesizefitsall pill for active PsA, but a toolbox of medications and lifestyle tweaks can keep the disease in check.
Pharmacologic Strategies
NSAIDs & Steroids
Nonsteroidal antiinflammatory drugs (like ibuprofen) can relieve pain for mild flares. Short courses of oral or injected steroids may be used for a rapid reset, but theyre not a longterm solution because of sideeffects.
DMARDs (DiseaseModifying Antirheumatic Drugs)
Methotrexate and leflunomide are the classic workhorses. They slow joint damage and can also improve skin lesions, but they require regular blood monitoring.
Biologic Agents
Biologics target specific parts of the immune system. The most common families are:
- TNF inhibitors (e.g., etanercept, adalimumab)
- IL17 blockers (secukinumab, ixekizumab)
- IL23 inhibitors (guselkumab, risankizumab)
Studies show that up to 70% of patients reach low disease activity within a year on biologics .
Emerging Therapies
JAK inhibitors (like upadacitinib) are oral options that show promise for patients who cant tolerate injections. Biosimilars are also becoming more affordable, widening access.
NonPharmacologic Strategies
Physical Therapy & Exercise
Gentle rangeofmotion exercises keep joints lubricated. Think swimming, yoga, or lowimpact cycling activities that wont aggravate inflamed joints.
Lifestyle Tweaks
- Weight management Extra weight puts extra stress on joints.
- Smoking cessation Smoking fuels inflammation.
- Stress reduction Mindbody techniques can lower flare frequency.
Discussion Checklist
When you next meet your rheumatologist, ask about:
- Which medication class best matches your disease activity?
- What monitoring labs are needed?
- How can we incorporate physical therapy into the plan?
- Are there any lifestyle changes I can start today?
Balancing Benefits & Risks
Every treatment carries a tradeoff. The key is to weigh shortterm relief against longterm safety.
Common SideEffects
- Infections especially with biologics and JAK inhibitors.
- Liver enzyme elevation a concern with methotrexate.
- Injection site reactions usually mild and brief.
LongTerm Outcomes
Effective control of active PsA can halt joint erosion and preserve function. However, chronic immunosuppression demands vigilance for infections and regular checkups.
DecisionMaking Matrix
| Therapy | Pros | Cons | Best For |
|---|---|---|---|
| NSAIDs | Quick pain relief | GI upset, limited effect on disease | Mild flares |
| DMARDs | Slows joint damage | Blood monitoring needed | Moderate disease |
| Biologics | High efficacy, skin improvement | Infection risk, cost | High activity or axial disease |
| JAK Inhibitors | Oral, fast onset | Thrombotic risk, labs needed | Patients preferring pills |
Living With Active
Managing active PsA isnt just about meds; its about weaving a lifestyle that supports joint health while still enjoying life.
Managing Flares
When a flare hits, start with a short course of NSAIDs, rest the affected joint, and apply ice. If symptoms persist beyond a few days, call your rheumatologist early intervention prevents escalation.
Work & Daily Activities
Ergonomic adjustments can make a world of difference. Consider a keyboard with a wrist pad, a standing desk that allows you to shift weight, or shoes with good arch support for those lingering foot pains.
Mental Wellness
Chronic illness can take a toll on mood. Connecting with support groups, whether online or in your community, can reduce feelings of isolation. Mindfulness meditation has been shown to lower perceived pain intensity.
Resource List
- Psoriasis Foundation patient education and mentorship programs.
- Arthritis.org symptom trackers and medication guides.
- Mobile apps like MyJointHealth for daily logging.
A Note on Curing PsA
Some people write headlines like I cured my psoriatic arthritis, but medically we talk about remission a state where disease activity is minimal and symptoms are controlled. Keeping realistic expectations builds trust and reduces disappointment.
Key Takeaways
Active psoriatic arthritis is a treatable, manageable condition when youre armed with the right knowledge. Early detection of the six hallmark signs, especially subtle foot symptoms, can prevent irreversible joint damage. Understanding the five disease patterns guides personalized treatment, whether you end up on a DMARD, a biologic, or a newer JAK inhibitor. Balancing medication benefits with potential risks, adding physical therapy, and adopting lifestyle changes creates a holistic plan that protects both joints and overall wellbeing.
Now that youve got the roadmap, why not take the first step? Book an appointment with your rheumatologist, ask the checklist questions, and start tracking your symptoms today. Your joints deserve the same care you give your skin and you deserve to live without unnecessary pain.
FAQs
What are the first signs that psoriatic arthritis is becoming active?
Early indicators include joint pain or tenderness after rest, persistent swelling, morning stiffness over 30 minutes, nail changes, red scaly skin patches, and enthesitis (pain at tendon‑bone insertions).
How does active psoriatic arthritis differ from remission?
During an active phase, inflammation causes noticeable pain, swelling, and stiffness, while remission means symptoms are minimal or absent and disease activity scores (DAS‑28, PASI) are low.
Which type of psoriatic arthritis is most likely to be “active” and cause severe symptoms?
Axial involvement (spine and sacroiliac joints) and dactylitis (sausage‑like swelling of fingers or toes) often produce the most pronounced active disease because they affect major functional areas.
What treatment options are best for controlling an active flare?
Mild flares may respond to NSAIDs, but moderate to severe activity usually requires disease‑modifying drugs such as methotrexate or biologics (TNF‑α, IL‑17, or IL‑23 inhibitors). Newer oral JAK inhibitors are also an option for those preferring pills.
Can lifestyle changes help reduce the frequency of active psoriatic arthritis flares?
Yes. Maintaining a healthy weight, quitting smoking, regular low‑impact exercise, stress‑management techniques, and ergonomic adjustments can lower inflammation and the likelihood of flares.